- 1A Systematic review of homogenous RCTs
- 1B Well-designed individual RCT
- 2A Systematic review of cohort studies
- 2B Individual prospective cohort study, low quality RCT, ecological studies; and two-group, non-randomized studies
- 3A Systematic Review of case control studies
- 3B Individual retrospective case-control studies; one-group, non-randomized pre-post test study; cohort studies
- 4 Case series (and low quality cohort and case control study)
- 5 Expert opinion without explicit critical appraisal
- * This was a systematic review which included mostly RCT’s and Level II studies. As this type of systematic review doesn’t fall into either 1A nor 2B, I chose to categorize it into a level 2A study. The evidence reviewed was higher than case studies but lower than cohort studies.
Methods
The authors of this systematic review included studies that investigated the effect of interventions that are not Ayres Sensory Integration specifically. They included studies published between 2007 and May 2015. Authors included studies on sensory-based techniques as well as sensory environmental modifications. Interventions targeted clients between 2-21 years old with sensory integration difficulties. Authors ensured that articles investigated specific sensory techniques or sensory environmental modifications.
Findings
Qi-jong massage The authors concluded there is strong evidence for young children with ASD with Qi-jong massage (Bodison, S.C. & Parham, L.D. 2017, p. 5).
Three Level I and and 1 Level II studies demonstrated improvements in self-regulation, parenting stress, tactile differences and ASD symptoms. Children were 2-7 years old and had ASD. Their parents, after being trained by occupational therapists, provided 15 minute daily massage. The studies lasted 4 and 5 months.
Important to note is that the OT’s had at least 50 hours of training in Qi-jong before training parents on its implementation. This may make it a challenge intervention for most OT’s to implement.
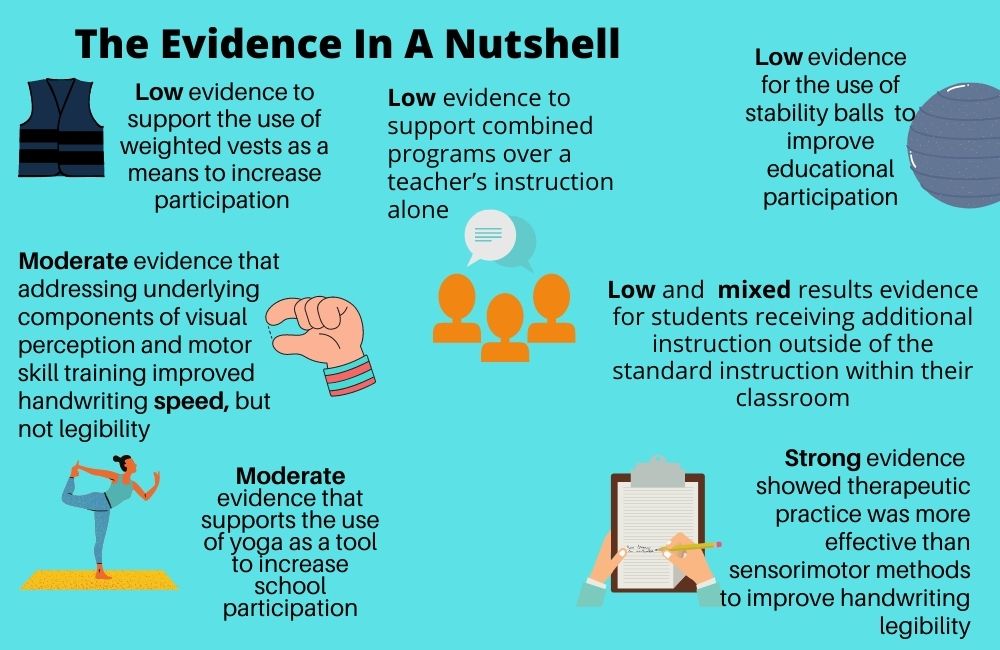
Weighted Vests The authors concluded there is limited evidence for the use of weighted vests for children with ADHD (Bodison, S.C. & Parham, L.D. 2017, p. 5).
A level I study did show improved attention and in-seat behavior when a group of 6-9 year olds wore vests with 10% of their body weight. The authors mention that limitations in the design of the study impacted its internal validity. This in turn caused them to interpret these findings with caution.
Study authors also noted that the evidence they found for the use of weighted vests with children with ASD had low levels of evidence, so these studies were not formally included in the review. The authors conclude the evidence for the effectiveness of weighted vests for children with ASD is insufficient at this time.
Slow Linear Swinging The authors concluded there is insufficient evidence to support the use of slow linear swinging to improve attention for children with ASD.
A level I study investigated the impact of being on-task following slow, linear swinging in a group of children with ASD. The study demonstrated no significant difference between children who swung and those in the control group (Bodison, S.C. & Parham, L.D. 2017, p. 6).
Study authors did note a limitation of this study is that the arousal level of children was not assessed prior to their participation in swinging. They posited, therefore, that if a child was in a low arousal state prior to a calming activity, this may have demonstrated no positive impact on the child’s on-task behaviors.
Sensory Enrichment in Preschool The authors concluded there is insufficient evidence supporting sensory enrichment in a preschool classroom.
This level I study investigated the impact of embedding tactile, proprioceptive and vestibular activities for 12 weeks in a preschool classroom’s daily routine. All children in the classroom participated in these activities, but one group of children also received ASI through OT sessions.
Both groups improved in their play skills, but no difference was noted between them. Study authors of this review mention that design limitations, including a very small sample size of 8, limit the implications of the study findings.
Sensory Environmental Modifications The authors concluded there is moderate evidence supporting sensory adaptations of a dental environment to assist participation for children with ASD in their routine dental cleanings (Bodison, S.C. & Parham, L.D. 2017, p. 6).
Children reported improved measures of pain intensity and sensory discomfort as well as improved participation in dental cleaning for typically developing children and those with ASD. Children received deep pressure from a decorative wrap and the auditory and visual aspects of the the dental environment (Bodison, S.C. & Parham, L.D. 2017, p. 7).
Most interesting to me is that investigators measured children’s electrodermal responses as a means to quantify impact on stress and anxiety. They found a moderate to large effect size for children with ASD after they received the intervention!
So What Do You Think?
I appreciate when studies have high standards for the research they include in their reviews. However, due to the nature of the current evidence in OT, that sometimes means there is limited information on the interventions we use most.
I’m interested in the idea of Qi-jong massage, but I will say that the skeptic in me thinks, “Well, if anyone received a 15 minute massage to start their day, I would definitely expect them to show improvements in their behaviors.” I also am curious to see if the massage was compared to other interventions such as a tailored sensory diet. If families really followed up with those every day with good fidelity, I hypothesize that we would similarly see as good if not better results in the developmental gains for children.
Reference
Bodison, S.C., and Parham, L.D. (2017). Specific Sensory Techniques and Sensory Environmental Modifications for Children and Youth with Sensory Integration Difficulties: A Systematic Review. American Journal of Occupational Therapy 72 (1). https://doi.org/10.5014/ajot.2018.029413