Do you have a sensory kid, or maybe you’re trying to figure that out? Finding out your child has sensory processing differences is usually step one. Then the journey of figuring out what to do about it begins. One of the most challenging parts of that journey can be finding what sensory tools work for your child.
“Sensory” is very widely found on Facebook, Instagram and Pinterest. But the thing is, it’s not as simple as trying whatever sensory activity you’ve pinned and now your child can deep breathe away their troubles.
So how do you figure out what will help your child to find their calm? To manage their frustration, cool down during a meltdown and get focused when they need to?
Here are my top 3 tips to figuring out your child’s sensory needs and loading up a toolbox of tools that you can easily access and use.
Observe observe observe. Spend time watching what kind of activities and things your child gravitates toward. Observe how they move. Do they like chill, calm music or music with a heavy, grounding beat (think reggaeton, rap). Do they like chewy and crunchy foods or prefer more smooth things? Hate getting their hands dirty or can’t wait to walk barefoot in the grass? These things will be useful for noticing trends.
Learn about the sensory systems. Once you have noticed what things your child loves and hates, you have lots of useful data. But, now you need to learn why your child getting overwhelmed in busy environments might actually have something to do with how they process movement. Or that the fact that they’re a little bit clumsy and run into doorways all the time might mean that they need some heavy work before or after they’re doing something that makes them anxious. If you already have a good understanding of the different sensory systems but need some low to no cost and easy to implement activities, one of my PDFs might be useful for you. If you have no idea what vestibular and proprioceptive processing are and want to know if they might help your child, my self-paced video class for parents has everything you need to know!
Pick tools that match your child’s preferences and sensory needs. This is where you will have your “aha!” moments. Knowing what activities your child likes and understanding the sensory reason why empowers you to choose activities that will provide the input they need to feel calm, happy and ready to learn.
Need more individualized help figuring out your child’s sensory needs?
Want to have a free 15 minute chat to see if your child’s needs are sensory based at all? You can book a free discovery call with me to help guide you to what step is next in helping you and your child find more peace and calm.
Sensory travel tools are worth a shot, because I feel like the challenge of traveling with kids is one of those life experiences that you don’t understand until you do it for yourself. I can at least speak for myself and say that a 9 hour car ride in the backseat with my 4 month old baby changed me 😅
Depending on your personality type, the actual act of traveling itself might feel like no big deal, or it might get you stressed just thinking about it 😳 There’s figuring out what clothes you need (or might possibly need. #chronicoverpackersunite), making sure you have enough snacks to manage your blood sugar levels and prevent hangry episodes, things to entertain yourself with on the trip…
But traveling with kids. That’s next level. Because now you have to use your fortune telling skills to try to anticipate someone *elses’s* needs on a trip. What snacks will they want, what activities will keep them entertained [I, for example, never expected a 1 L water bottle to be the MVP of road trips, but I periodically remind my husband to not throw it out because it has proved its worth in gold multiple times no2w], what clothes will be comfy for them to travel in. So let me first give some general sensory tips to consider for traveling, and then I’ll share some sensory tools that can be useful for family trips.
Structure The Trip to Meet Sensory Needs
Let your child decide what clothes to wear. Obviously if you are dressing all your kids in a certain color so you can easily identify them, stick with the plan. But make sure it’s something they’re comfy in.
Make sure to have good meals and have plenty of snacks! I think this is something that most parents know, but I think we can sometimes get so stressed by trying to get all of our stuff and all of the people through security/in the car/on the train etc etc in time and your child starts having a meltdown when you realize, “Oooh. We haven’t eaten since breakfast 4 hours ago.” 😳
Speaking of snacks…Especially if your child likes crunchy or chewy snacks, make sure to pack some for some good, calming oral motor input. Just be mindful of snacks that could be a choking hazard while they’re eating in the car. Another great way to fit in some oral motor input while traveling is using water bottles with straws.
Consider playing music with a heavy beat for kids who get carsick/motion sickness. Music is a very powerful sensory tool. And if your little one (or big one) gets motion sickness? Often times music with a very grounding, heavy beat (like reggae, reggaeton, rap, country) can be very calming and help them to feel more connected to their body (when they feel disconnected is part of how motion sickness happens).
Be prepared to take breaks where they can move around. As best as you’re able, allowing your child to climb around for 10 minutes at a rest stop, get some spins in or walk or crawl up or down the aisle on a plane…little kids’ (particularly sensory kids’) brains are wired for movement so they crave it, and get a little more grouchy, hyper, emotional, etc. when they don’t get it.
Now onto the tools…some are very simple and very old school (which I’m a fan of.) I very much subscribe to the idea that you don’t need to spend a bunch of money to meet a child’s sensory needs. *However* I’m also going to include some fun/nifty/unique items that I think are worth getting if you are interested in them.
Pom poms. I said old school, right? These little guys are great because they’re quite portable (can stick them in a pocket, purse, backpack…) and they’re a great physical/tangible tool if you want to get some breaths in. Taking calming breaths rarely works for many of the sensory kids I know. A lot of sensory kids really require hands on tools for learning, and trying to breathe requires a lot of body awareness that many just don’t have. But if you add a pom pom to the mix, you might get some breaths! Blow them across the tray on an airplane for self regulation, or just some fun 🙂
Bubbles: For the same reasons as pom poms…you can get some breaths in using a prop if your child can blow from the bubble wand. Alternatively, these are great for kids who like visually interesting things. Speaking of which…
Sand or gel timers: These are great for kids who love visually captivating things. They can be used to actually track time or to just watch the sand or gel trickle down. They’re nice and portable also, which makes them a great sensory travel tool.
Wacky Track Fidgets: These are a nice, travel-sized heavy work activity for your child’s hands. Heavy work is generally calming for everyone. Using your hands to work against resistance can fit in some nice heavy work, and these links that click when you snap and manipulate them can work that in to your child’s travel time.
Floam: Obviously most textured sensory mediums are way too messy to take on trips, but I think Floam is worth a shot for a sensory travel item. The texture is kind of like a non-edible version of rice crispy treats. It pulls and pushes apart and has a slightly sticky aspect to it. You can squish it up and easily form it into shapes for sculpting etc, or just use it like a stress ball and squish to your heart’s desire. It’s not crumbly like kinetic sand and it shouldn’t squish into things like carpets etc.
Squigz: What’s a sensory toys/tools list without Squigz? Just kidding–kind of. These are just fun and intriguing. They also provide some of that heavy work for your hands I mentioned with the Wacky Track Fidgets. They stick onto basically anything, and the hard work of pulling them apart is fun and can use up some energy. The standard size ones are kind of big to take many of on a plane, but they also have mini ones available. These might be best suited for slightly older kids (manufacturer info says 5 years old) because they could be too hard for little hands to pull.
Noise cancelling earbuds/headphones: These are a great tool to have on hand for kids who get easily overstimulated by noises. The noise deafening are great for children [or parents] who want to still participate in convos but just need things to be toned down a bit.
Headphones for music: Alternatively, you might have a child who really is soothed by music, so having their own set of headphones to listen to music while traveling can be supremely helpful. Work with your child to decide if ear buds or over ear headphones are best.
Eye mask: this may be my personal bias, because I am *very* sensitive to light. But if you’re traveling (particularly on a plane or train) during times when your child might need to sleep and they’re sensitive to light, an eye mask might help them a bit. It is also useful to have in the event that wherever you’re staying is brighter than home and your child struggles to fall asleep that way.
Snack box: This is part sensory but also part fun and motor. This is just a fun way to expand the time your child takes to work through all those yummy snacks you packed.
There you have it! My top 10 sensory recommendations for sensory travel. I hope something strikes you as helpful for your child and that you can feel a bit more empowered as you prepare to travel with your littles in tow!
Sensory processing is so central to what peds OT’s do these days, but there remains a lot of difference in opinions. From “whether it exists,” to what’s the most effective way to treat it. One often leaves OT school feeling like there’s still a lot of new learning to be done.
Learning curves for new grads can be steep. I will say that I personally have shifted my thinking dramatically as an OT since the time I graduated. I have gone from being verydetail oriented, goal focused, everything must look like typical to much more practical, holistic and functional.
This journey has led me to be interested in developmental approaches like the DIR/Floortime model. From what I’ve read, it is a collaborative approach between parents and professionals, in which parents are key players. It also emphasizes emotional development and engagement. These are also two elements that have become largely more important to me as I’ve learned to see the forest instead of focusing only on the trees.
I plan to research more into DIR and similar approaches, but this was a basic starting point on an article that reviewed DIR’s impact on communication and self-regulation.
Journal Journal of Occupational Therapy, Schools, & Early Intervention (SNIP 0.535)
Article Title Intervention effects on communication skills and sensory regulation on children with ASD
4 Case series (and low-quality cohort and case control study)
5 Expert opinion without explicit critical appraisal
Methods Professionals recruited 25 children aged 3-6 years old with ASD and their families to participate in this study.
Intervention
A multi-disciplinary team developed focused individualized intervention plans for each child that were completed for a 10 month period. The programs included 1-2 elements that were included in the approach: Floortime, sensory integration and speech therapy (Helena I. S. Reis, Ana P. S. Pereira & Leandro S. Almeida p. 349, 2018). Important aspects of the intervention process included:
A team of multi-disciplinary professionals who worked as a team with families
Identifying children’s strengths, preferences and interests
Focusing on developmental areas that emphasis connection, engagement and social skills to promote learning in a child’s natural environments
Every member of the team of professionals was trained in DIR/Floortime and OT’s additionally were trained in Ayres Sensory Integration (Helena I. S. Reis, Ana P. S. Pereira & Leandro S. Almeida p. 350, 2018). All team members had also worked for more than 5 years in the Early Intervention System with children with ASD.
Sessions were as follows…
Floortime A psychologist led parents in 30 minute Floortime sessions, in which psychologists coached parents in promoting joint attention from their child. The psychologist also observed and provided feedback to the parent utilizing these skills following the time spent working together.
Sensory Integration OT’s led sessions for 30 minutes if the child participated in multiple therapies from the three options (SI, Floortime and Speech therapy). The children who only participated in SI therapy participated in 45 minute sessions. OT sessions aimed to promote joint attention, social skills, perceptual skills and motor planning through eliciting increased integration of sensory input.
OT’s also provided education to parents as to the connection between sensory integration abilities and difficult behaviors children sometimes display. In this education, OT’s included information on how to adapt the child’s every day routine with modifications to promote regulation.
Speech Therapy Speech therapists used augmentative and alternative communication systems in sessions to promote natural gestures and symbolic communicative forms during their 30 minute sessions (Helena I. S. Reis, Ana P. S. Pereira & Leandro S. Almeida p. 352, 2018).
Measures Parents completed the Assessment Scale of Children with ASD, which gathers information on Social Communication, Repetitive Behaviors and Restricted Interests, and Sensory Processing.
Findings
Children demonstrated statistically significant improved scores for the areas of Social Communication and Sensory Processing. The area of Repetitive Behaviors and Restricted Interests did not yield a statistically significant in the change in parents’ ratings.
Things to Consider
The authors note that the study had no control group, so the results cannot be compared to a lack of treatment, alternative treatment, nor control for development by maturation alone. They also noted that they did not compare or categorize children based upon the severity of their symptoms of each area included.
A limiting element in applying this study to a wide array of OT’s is that the OT’s in this study were trained in both Ayres Sensory Integration and Floortime. I definitely believe I do Sensory Integration Therapy based on the principles in the infographic above, but I’m not officially trained. What I do take away from this article is evidence that developmental models such as DIR/Floortime are a valuable tool to enhance the occupational therapy one is already providing.
References
Helena I. S. Reis, Ana P. S. Pereira & Leandro S. Almeida (2018). Intervention effects on communication skills and sensory regulation on children with ASD, Journal of Occupational Therapy, Schools, & Early Intervention, 11:3, 346-359, DOI: 10.1080/19411243.2018.1455552
Watling, R., & Hauer, S. (2015). Effectiveness of Ayres Sensory Integration® and sensory-based interventions for people with autism spectrum disorder: A systematic review. American Journal of Occupational Therapy, 69, 6905180030.
Hand skills and how they develop in infants are so intricate and fascinating. I worked only a brief stint in early intervention, so my exposure to working with infants has been limited. I love babies, but I have always thought I would have to be more seasoned to be a therapist to infants. My fresh out of the gate, type A, overachieving new grad self struggled with the fact that one can hardly make babies do what you want them to do! Now that I’ve had some time to learn how to finesse and scaffolding activities for older kids, I think I would have a better go with babies too.
This article was interesting to me because I loved the idea of constraint induced movement therapy when I learned about it. Not because I love restricting a child’s movement, but the concept just makes good sense to me.
What I love even more about this article, though, is that they were detail oriented. They don’t argue that CIMT and mCIMT don’t benefit children with cerebral palsy. However, they specifically wanted to know how it might impact outcomes for infants with CP.
Journal American Journal of Occupational Therapy (SNIP score 1.121)
Article Title Effectiveness of Modified Constraint-Induced Movement Therapy Compared with Bimanual Therapy Home Programs for Infants with Hemiplegia: A Randomized Controlled Trial
4 Case series (and low-quality cohort and case control study) [This study was a cross-sectional study]
5 Expert opinion without explicit critical appraisal
Methods Health professionals recruited parents through public health services. Children could be included if…
They had a formal diagnosis of spastic hemiplegic CP from a physician
They were 8-16 months old (no older than 18 months at the end of treatment)
Could follow simple and age-appropriate instructions
Researchers excluded children with additional medical issues and those who demonstrated no difference in the function between their two hands. Study authors randomly assigned children to either a modified Constraint Induced Movement treatment group or a Bimanual Therapy group. Thirty three infants and their families participated in 8 weeks of individualized daily one-hour play sessions 7 days per week. Occupational therapists visited the families once per week and guided parents on ways to promote the child using his/her affected hand during play.
Intervention
Children in the mCIMT group wore a soft, custom-made mitt and participated in activities to promote unilateral hand use. The children in the BIM group completed activities to encourage symmetrical and asymmetrical hand use. All children had sufficient head control, and treatments were done with the child sitting (floor or high chair) and given trunk support if needed.
During weekly visits, the OT’s ensured that parents knew to provide positive reinforcement for desired actions when performed. The professionals also guided parents on the activities they should complete the following week. The researchers required parents to complete a daily log with details of the play sessions.
Measures
Researchers used the Mini-AHA, which is an infant version of the Assisting Hand Assessment. This assessment uses criterion reference to measure the effectiveness of 8-18 month olds with hemiplegia’s use of their affected hand (Chamudot, R. et al, 2018, p. 2). Evaluators observe infants playing with specific toys which promote the use of bilateral hands. The scores on the Mini-AHA are not influenced by age.
Researchers also developed a Functional Inventory as a means to measure the results the treatment program had on gross motor and hand function for infants 7-18 months old. The FI has 31 items and is divided into Gross Motor Skills, Unilateral Hand Use and Bilateral Hand Use (Chamudot, R. et al, 2018, p. 3). The authors found high internal consistency for the initial total FI score, post-treatment total FI score and the three categories.
Parent Completed Measures
Parents completed the Dimensions of Mastery Questionnaire which measures infants’ mastery of motivation (Chamudot, R. et al, 2018, p. 4). Parents also provided information about pregnancy and labor in addition to demographic information.
Findings
Parents in the mCIMT group completed an average of 48.4 hours (out of 60 total for the intervention), and parents in the BIM group completed 45.0 hours on average.
Investigators found there was a significant main effect with large effect sizes of time on all of the outcome measures (Chamudot, R. et al, 2018, p. 6). Children in both groups demonstrated higher scores after treatment. When investigators assessed the interaction of time with treatment and effects of treatment, the results were insignificant. Researchers found significant and equal improvement gross motor function from analysis of the FI.
Authors investigated the interaction between motivation (from the parent reported scores on the DMQ motivation questionnaire) and performance. They did find one significant interaction with a medium effect size. Children in the mCIMT group (though not those in BIM) who scored low on the Object Oriented Persistence subscale of the DMQ at baseline, showed significantly greater improvements.
Authors posited that perhaps children with lower motivation to engage in tasks with their hands may benefit more from mCIMT than children with similar physical presentation but high motivation to engage objects with their hands prior to treatment.
Things to Consider
The authors mentioned that there was no control group that did not receive treatment to compare to the interventions. However they also mentioned that this practice could be viewed negatively because early intervention can have such a large impact on children’s development. To deny them treatment in this crucial window intentionally could reap long lasting detriment.
Important to note is that this article specifically sought to determine what difference, if any, investigators would find in comparing two treatment interventions for infants with spastic hemiplegia. There is evidence indicating the benefits of CIMT and mCIMT for children older than two years. So, it is important to differentiate and consider the differences between infants and older children when selecting treatment interventions.
References
Chamudot, R., Parush, S. Rigbi, A. Horovitz, R., & Gross-Tsur, V. (2018). Effectiveness of Modified Constraint-Induced Movement Therapy Compared with Bimanual Therapy Home Programs for Infants with Hemiplegia: A Randomized Controlled Trial. American Journal of Occupational Therapy 72 (6): 7206205010. https://doi.org/10.5014/ajot.2018.025981
Feeding therapy. I always say it’s a love-hate relationship for me. It’s love because I myself love food and eating. My Italian side of the family is big into cooking, so food definitely is a large part of our culture, and many cultures.
I love seeing kids become more confident and enjoy the process of exploring new foods and flavors. I think it’s fun to be silly with them and talk about taking shark bites vs. mouse bites, seeing who can crunch a carrot the loudest, etc.
The hate side of things isn’t so much a hate as it is a frustration that stems from my impatience. I am through and through a bottom up thinker. I have a hard time not getting to the root of an issue because I feel any progress we’ll see otherwise is likely a temporary bandaid. The struggle I have with feeding therapy is that a child can make lots of progress in the clinic, but seems to have a stand still at home.
As time has gone on, I firmly see that feeding therapy is whole family therapy. That’s not a bad thing, and really every therapy should be that way! However, there are so many emotional dynamics that go into mealtime that unlike learning to cut with scissors, if you don’t somewhat address the bigger emotional dynamic, you’ll likely see very limited progress.
This week’s article is to highlight the connection between family dynamics and feeding outcomes. So while the article doesn’t tell you what to directly do, (although I did write a review that covers that subject) I wanted to review it as a means to support the idea that addressing family dynamics is crucial in feeding therapy.
Journal Eating Behaviors (SNIP score 1.106)
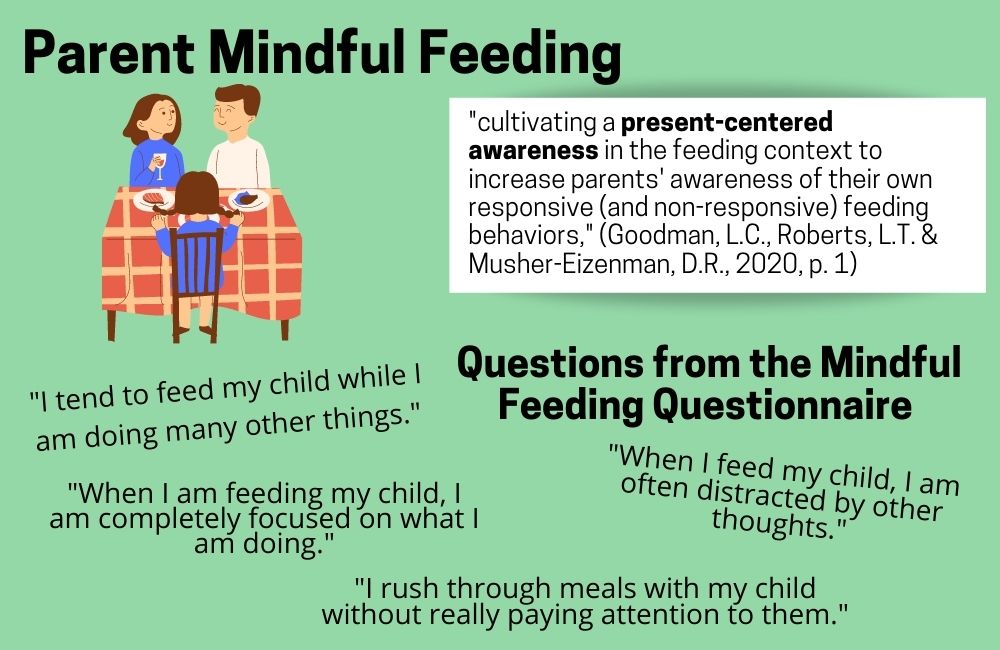
Article Title Mindful Feeding: A Pathway Between Parenting Style and Child Eating Behaviors
4 Case series (and low-quality cohort and case control study) [This study was a cross-sectional study]
5 Expert opinion without explicit critical appraisal
Methods Researchers recruited 496 parents from a sample of a larger study on the topic of feeding. Parents completed an online survey.
Measures
Mindful Feeding Study authors used the Present Centered Awareness subscale of the Mindful Feeding Questionnaire to determine parents’ mindful attention during the process of feeding their children.
Child Eating Behavior Study authors used subscales from the Child Eating Behavior Questionnaire as a means to measure children’s emotional over-eating and food fussiness per parent report.
Problematic Mealtime Behaviors The Problematic Child Mealtime Behaviors subscale of the Meals in Our Household questionnaire served as a tool to gather parent report on mealtime behaviors.
Parenting Style Investigators used the Parenting Practice Questionnaire to serve as a tool to classify parents’ parenting style as authoritative, authoritarian or permissive.
Findings
In general, the parents who self-reported more authoritative parenting reported higher levels of mindful feeding, while those reporting more authoritarian and permissive parenting reported less mindful feeding (Goodman, L.C., Roberts, L.T. & Musher-Eizenman, D.R., 2020, p. 3). Those parents who used mindful feeding strategies more often had children who they reported were less likely to be fussy, less likely to eat in response to emotions and less likely to have problematic mealtime behaviors ((Goodman, L.C., Roberts, L.T. & Musher-Eizenman, D.R., 2020, p. 4).
Authoritative Parenting Per parents’ self-reports, authoritative parenting had a direct and indirect negative impact on children’s emotional over-eating and food fussiness. Meaning, those with an authoritative parenting style had children who were less likely to be fussy and to eat as a reaction to their emotions. This style of parenting did not demonstrate a negative direct impact on problematic mealtime behaviors.
However, when authors assessed how authoritative parenting impacted mindful feeding and how that in turn impacted problematic mealtime behaviors, they did find a significant effect. So, having an authoritative parenting style doesn’t directly impact mealtime behaviors. However, an authoritative style impacts a parents’ mindful feeding habits, which in turn impacts the problematic mealtime behaviors.
Authoritarian Parenting Per parents’ self-reports, authoritarian parenting had a direct and positive impact on children’s emotional over-eating. That is, parents with an authoritarian parenting style reported their children as more likely to eat in reaction to emotions. This result was not seen for food fussiness and problematic mealtime behaviors. As authors assessed how authoritarian parenting impacted mindful feeding and how that in turn impacted problematic mealtime behaviors, food fussiness, and emotional over-eating, they did find a significant effect.
Permissive Parenting Parents who self-reported permissive parenting style had both a direct and indirect positive impact on problematic mealtime behaviors, food fussiness, and emotional over-eating. This means, parents reporting this style also reported their children as presenting with more mealtime behaviors, food fussiness and emotional over-eating.
Things to Consider
The authors mention that it would be beneficial to the research to complete a longitudinal study in which they could assess these outcomes for the same group of parents and children at multiple points in time. This would allow drawing stronger conclusions about the connection between parenting style, parents’ mindful feeding habits and children’s eating behaviors.
Of note is that the sample in this study had a majority demographic of white families (79%), which may impact the ability to generalize findings to the picky eating population. I was not able to find the race demographics for picky eaters, so I can’t conclusively say one way or another.
The study authors also mention that it would be valuable to explore the bidirectional relationship between parents’ mindful eating habits and children’s challenging behaviors, as the children’s challenging behaviors may also impact the parents’ strategies. Finally, they include that exploring other factors, such as other life stressors, that may impact this relationship between parent and child dynamics during feeding would be useful.
What does this all mean for a feeding therapist?
While this data is preliminary and low level evidence, I think it is very important to acknowledge and include families in feeding therapy intervention. I think we are doing a disservice to children and their families if we expect the child’s progress in the comfort of a therapeutic feeding session to transfer over to home without directly also educating parents and caregivers on how to interact with food, respond to their children and shift a mindset of learning to learn about food.
References
Goodman, L.C., Roberts, L.T., & Musher-Eizenman, D.R. (2020). Mindful feeding: A pathway between parenting style and child eating behaviors. Eating Behaviors 36. http://doi.org/10.1016/j.eatbeh.2019.101335
Telehealth has drastically changed the way many therapists are practicing in these past six months. (Six months! Can you believe that?) I haven’t personally tried my hand at it because I was let go from my job when COVID closed schools and clinics in March. I am always eager to hear my former coworkers talk about their experiences navigating the unchartered waters of telehealth. I’ve also admired the creativity, ambition and flexibility as I see resources, tips and tricks that therapists new to telehealth have discovered and shared.
Adapting to Telehealth Like Champs
I may be biased, but therapists are incredible people. While the adaptability, creativity, goal setting and executing that many bring to the field has made providing telehealth services possible, I have to believe many are grieving the loss of in person therapy. I’m getting married and moving abroad in a month or so, so it didn’t feel like the right timing for me to get a new job. However, I have thought about how I hope to get an OT job when I move. I’ve had to tell myself that I might have to be open to telehealth if that is what my option ends up being, and that makes me so sad.
But, alas, accept the current state of society we must. My goal in covering this topic is to encourage people doing telehealth that what you’re doing can make a difference! I know I’ve heard many people say, “It’s not really effective.” I can certainly imagine that, if the parents aren’t involved. There are often factors we can’t control. However, there are always things that are within our power to change.
How to Provide Effective Telehealth OT Services
I’m hoping this article review serves as encouragement that doing the hard work to shift our thinking even more from “I’m the therapist and I’ll make the change,” to “We’re working as a team and my collaborating with the caregivers will help this child to continue to succeed,” is worth it. You will also find some specifics and direction of elements that the investigators in this study used in order to promote successful parent coaching.
JournalThe American Journal of Occupational Therapy (SNIP score 1.121)
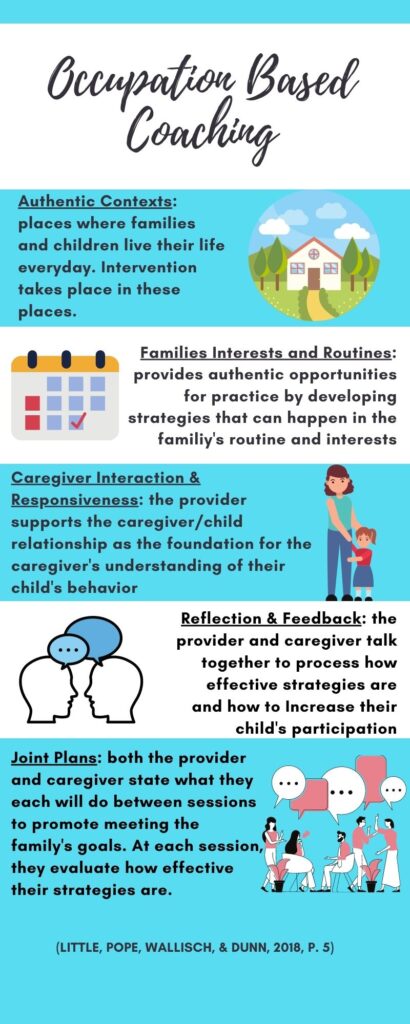
Article Title Occupation-Based Coaching by Means of Telehealth for Families of Young Children with Autism Spectrum Disorder
Authors Lauren M. Little, Ellen Pope, Anna Wallisch, Winnie Dunn
4 Case series (and low-quality cohort and case control study)
5 Expert opinion without explicit critical appraisal
Methods
The study investigators recruited children in underserved and rural areas through early intervention and early childhood programs. Investigators included children with an Autism Spectrum Disorder who were 0-6 years old. Seventeen families completed the intervention.
Intervention
Occupational therapists completed 12 weeks of coaching sessions through Zoom. Therapists used the coaching model to empower families to understand and grow confident in the knowledge they have in regards to their child. The therapists ask questions to promote reflection, guide families to realize what knowledge they already have and use, as well as to guide families in developing and implementing strategies to assist their children in meeting goals the family set.
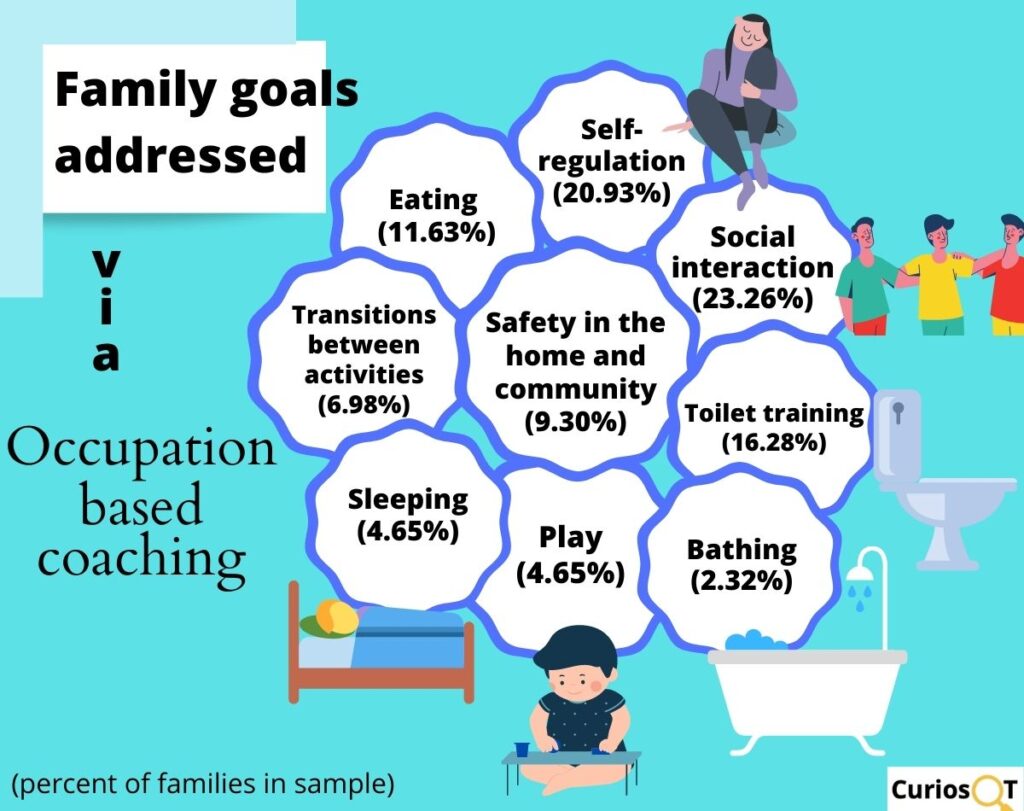
OT’s used the first session to complete a routine-based questionnaire as a means to gather information on the family’s daily routines and context of their daily activities. The family then came up with goals for the OT sessions. Investigators used the following measures to gather relevant data for the intervention.
Demographic Form-Family
Sensory Profile-Second Edition
Social Responsiveness Scale-Second Edition
Parenting Sense of Competence Scale
Assessment of Preschool Children’s Participation
Canadian Occupational Performance Measure-Second Edition
Study authors also used Goal Attainment Scaling to work with parents in establishing goals. This is a documentation method that uses established, sensitive levels of change for a targeted goal to demonstrate progress in that area.
Findings
Authors compared the mean scores of each measure from pre and post intervention to determine the effects of intervention.
Parent Efficacy as a Result of Telehealth Coaching
Post-intervention scores for the Parenting Sense of Competence Scale (PSOC) demonstrated a significant increase in parents’ feelings of efficacy. This indicates that parents felt more equipped and able to manage the situations they encounter as a parent. Parents did not report increased levels of satisfaction. Satisfaction included the degree to which a parent reports their role as a parent is comfortable and rewarding (Little, Pope, Wallisch, & Dunn, 2018, p. 4)
(Little, Pope, Wallisch, & Dunn, 2018, p. 4)
Child Participation as a Result of Telehealth Coaching
The authors measured child participation with the Assessment of Preschool Children’s Participation (APCP), GAS goals and COPM-2. The frequency with which children participated in activities and the diversity of the activities in which children engaged significantly increased per the APCP. There was also a significant increase in parents engaging in more play activities with their children as well as trying a wider variety of activities to develop their child’s skills (Little, Pope, Wallisch, & Dunn, 2018, p. 5).
Children’s increased participation in activities was significant per data from the COPM-2. Parents’ satisfaction with intervention goals increased significantly, and children made significant gains in their GAS goals.
Things to Consider
The study authors mention that only parent report measures were used to gauge effectiveness of the intervention. They suggested that the addition of objective measures of behavior or performance may enhance understanding of coaching on child performance outcomes. They also mentioned that the use of a control group may be helpful to further understand the effectiveness of telehealth vs. other modes of service or no intervention. Finally, the need for a larger sample size was mentioned.
Experiences of Parents of Children with ASD to Guide Telehealth Intervention for Others
While the current study included only parents of children with ASD, I think this information serves as a good guide for coaching a wide variety of parents. A factor that is relevant to me is that these families lived in rural or underserved areas. There may be cultural differences for families with whom we are working who are receiving telehealth services due primarily to COVID. Most notably, I think of families in suburban or urban areas that may fill their schedules more than what I often see as a slower pace of life in rural areas. However, the fact that families were able to effectively use technology to participate at a distance and make significant measurable change is encouraging.
How is your experience with telehealth going?
Have you had to switch to providing telehealth this past year? What tools and resources are you finding helpful?
References
Little, L. M., Pope, E., Wallisch, A., & Dunn, W. (2018). Occupation-Based Coaching by Means of Telehealth for Families of Young Children With Autism Spectrum Disorder. American Journal of Occupational Therapy,72(2). doi:10.5014/ajot.2018.024786