Last week I reviewed an article that investigated the relationship between preschoolers with sensory over-responsivity and school-age anxiety disorders. The authors found a significant correlation between the two factors. Now we know that sensory over-responsivity may contribute to clients who present with anxiety. The next question is, “What is my role in treating childhood anxiety as an occupational therapist?”
It intrigues me that despite OT’s mental health origins, I don’t want to overstep and treat a child with anxiety. Using the Zones of Regulation curriculum has equipped me to help a child who presents with generalized anxiety and self-regulation troubles.
When It’s More Than Anxiety
I personally feel that when I sense a bigger family dynamic, it’s time to refer to a family counselor. Also, I see that many professions are supporting trauma informed care. I believe [read: my opinion] to work with children with more complex psychological involvement, we have an obligation to pursue continuing education in that realm and/or know when it’s time to refer out.
OT’s Role in Treating Childhood Anxiety from AOTA’s Perspective
Let’s see what AOTA has to say. In its Anxiety Disorders fact sheet, AOTA mentions that anxiety impacts children’s participation because the fears they may have of failing, interacting with others, or more intense factors like panic attacks may cause children to limit the activities they are willing to participate in.
They next point to the cycle of how not being able to participate in these activities can lead to low self-esteem and impact their habits and routines. This is totally the stuff of OT! Also very interesting to me is children not knowing what activities to do to relax. This seems especially important in the age of technology when it’s way too easy to do everything online. We as OT’s know that occupations we do with our hands promote mental health!
Alright, now that we know where OT can help children in managing their anxiety, what action steps we can take?
Action Steps for OT’s to Address Anxiety
At home OT’s help the child and family in establishing routines, educating family members on how anxiety presents and how it impacts a child’s engagement in activities. An OT can also help a family to find activities they can enjoy together to promote balance and relaxation.
An OT at school may similarly provide information to staff on how anxiety may impact a child’s participation. OT’s also can present ideas for how to structure a child’s day and strategies to assist with regulation. An OT may also promote presenting activities in a modified way to reduce anxiety.
The AOTA fact sheet recommends that an OT can help on the community level by offering education and ideas of how to cope with anxiety symptoms to organizations that involve parents and work with youth.
What’s Your Next Move?
Knowing that AOTA recommends the above in treating children with anxiety, what will you do differently the next time you join a child and family on their journey with anxiety?
References
Occupational Therapy’s Role in Mental Health Promotion, Prevention, & Intervention With Children & Youth Anxiety Disorders. Retrieved July 20, 2020, from https://www.aota.org/~/media/Corporate/Files/Practice/Children/SchoolMHToolkit/Anxiety
We’re all overly familiar with the phrase, “sensory or behavior,” but I think we may leave important factors out when we pit the two as an “or” situation as well as the connotation of what “behavior” means to us. Behavior, while simplified by an Antecedent, Behavior, Consequence model can seem straightforward, is often just the opposite.
What impacts a child’s behavior? So. many. things. We know that physiological factors like blood sugar and being tired impact it. We also know that emotional processing and patterns shaped by dynamics at home and with caregivers impacts it. Communication skills, especially an impairment of, guide behavior.
Today’s review explores a study that investigated the relationship between sensory processing and anxiety. A CuriosOT follower on Facebook requested that I explore this topic, and I was happy to do so as this is a topic I’ve wondered about myself in recent years.
In our busy society, I think we can see that more adults and children alike are presenting with mental health concerns. As an OT I know that I have seen kids who may have sensory issues, but definitely have anxiety. Other times I’ve seen children who seem to me that they obviously have anxiety, and I’m not sure if sensory processing is contributing to their challenges in occupational performance.
So, are sensory processing and anxiety related? Either way, what is OT’s role in treatment when we receive a child who has one or both of these diagnoses? Today’s post will cover the relationship between sensory processing and anxiety, and my next post will cover what is OT’s role.
Journal Journal of Abnormal Child Psychology (SNIP score 1.759)
Article Title Sensory Over-Responsivity: An Early Risk Factor for Anxiety and Behavioral Challenges in Young Children
4 Case series (and low-quality cohort and case control study)
5 Expert opinion without explicit critical appraisal
Methods
The study authors obtained their baseline sample from the larger sample of the Duke Preschool Anxiety Study. That study had three parts: screening, in-home assessment and a laboratory phase (Carpenter et al., 2018, p. 4). The sample from the Duke Anxiety studied was obtained by screening children between 2-5 years old during visits to their primary care clinics. The sample was found to be representative of the general population.
Authors of the Duke Anxiety study invited the children who met criteria for generalized anxiety disorder (GAD), separation anxiety disorder (SAD) and/or social phobia to participate in the Phase 3 laboratory assessment (Carpenter et al., 2018, p. 4). Authors of the current study recruited children from this phase 3 to participate in the Learning About the Developing Brain (LABD) study. This was a five year study in which researchers followed a group of 191 children to assess relationships between sensory processing during preschool years and anxiety during school-age years.
Assessments
Study authors used the Preschool Age Psychiatric Assessment to assess anxiety and sensory over responsivity characteristics. Parents completed interviews to assess for symptoms of a variety of psychiatric disorders for children of preschool age. Parents of 191 children completed this assessment when their child was in preschool and age at school-age.
Anxiety
Researchers classified children as either meeting impairment and symptom criteria for the included anxiety disorders (GAD, SAD and/or social phobia) or not meeting those criteria. Children were identified as positive on the anxiety screening if their parent included at least 4 of 10 items on the screening tool.
Sensory Over-Responsivity
Researchers used the PAPA at baseline and follow-up to assess sensory over-responsivity. Responses to the following sensory experiences were accounted for: 1. physical contact with other people 2. Contact with fabrics, clothes tags, etc. 3. Contact with food textures 3. Visual experiences 5. Auditory experiences, including loud or high-pitched noises 7. Olfactory experiences 7. Tastes 8. Sensations of motion 9. Any other sensory experiences.
Behavioral Challenges
This study highlighted sleep problems, GI problems, food selectivity and irritability as related behavioral challenges.
Findings
Sensory Over-responsivity is not Uncommon for Preschool Children
Twenty percent of parents reported at least one sensory domain as over-responsive from the pre-school sample (Carpenter et al., 2018, p. 8). The most commonly rated areas were tactile (18%) and auditory (4%). Children with sensory over-responsivity at preschool who remained rated as such by school-age was 56%.Sixteen percent of children whose parents did not rate them as sensory over-responsive in preschool were rated as having sensory over-responsivity by school-age.
The proportion of females who parents described as sensory over-responsive was higher than the proportion of males who parents ranked as so (Carpenter et al., 2018, p. 8). Parents of children whose children were categorized as below the federal poverty line also were significantly ranked more often as sensory over-responsive.
Relationship Between Sensory Over-responsivity and Anxiety Disorders in the Preschool Sample
Researchers found a significant relationship between sensory over-responsivity and anxiety diagnoses in preschool, as 43% of children who were categorized as sensory over-responsive also demonstrated criteria of anxiety disorder. Researchers found that there was also a significant relationship between sensory over-responsivity and other disorders (i.e. ADHD) from the preschool sample (Carpenter et al., 2018, p. 9).
Did Sensory Over-responsivity in Preschool Predict Anxiety Symptoms by School-age?
The authors found that sensory over-responsivity in preschool significantly predicted anxiety symptoms by six years old. This stayed true when other potentially confounding variables (including sex, age, race, poverty status) were accounted for. This also remained true when the factors of a child having sensory over-responsivity by school age, anxiety symptoms when in preschool and a diagnosis of other disorders in preschool were accounted for. All this to say that potentially confounding factors assessed for in preschool did not otherwise explain the development of anxiety by school-age.
What Type of Anxiety Disorder Does Sensory Over-responsivity Predict?
The authors found sensory over-responsivity as a significant predictor only for generalized anxiety disorder, not separation anxiety disorder or social phobias.
Could Preschool Anxiety Cause School-age Sensory Over-responsivity?
A child having anxiety symptoms in preschool did not significantly predict a presence of sensory over-responsivity in school age children. When researchers assessed if preschool sensory over-responsivity predicted non-anxiety disorders for school age children, they found it did not. This indicates that preschool sensory over-responsivity is a significant predictor specifically of anxiety for school age children as opposed to a wide variety of non-anxiety disorders.
So What’s the Link Between Preschool Sensory Over-responsivity, School-age Anxiety and the Behavioral Challenges We See by School-age?
Researchers found a significant relationship between preschool children with higher levels of sensory over-responsivity showing higher levels of anxiety by school-age. They also noted that school-age children with higher levels of anxiety have higher incidences of irritability and sleep problems. Researchers did not find a significant relationship between the sensory and anxiety measures as they impacted GI symptoms or food selectivity by school age.
Things to Consider
The authors mention that they only collected data for two periods of time which is insufficient to completely achieve the ideal statistical criteria to state the impact sensory over-responsivity has on how anxiety and behavioral challenges manifest.
The authors also mentioned that to measure sensory over-responsivity they used an interview that was comprehensive and not specific to sensory over-responsivity. They feel it may be best to use a tool that specifically measures that.
Also of note is that the measures for anxiety and over-responsivity came exclusively from parent-report. It would be beneficial to have a second rater to corroborate these levels. They also mentioned that research has shown that sometimes a mother’s emotional symptoms impacts her rating of her child’s symptoms of mental health conditions.
The researchers would also like to assess how sensory under-responsivity and sensory seeking relate to anxiety.
What Do You Think?
How do you decide if a child presents with anxiety or sensory processing disorder? How would you use this information to guide your treatment?
References
Carpenter, K. L., Baranek, G. T., Copeland, W. E., Compton, S., Zucker, N., Dawson, G., & Egger, H. L. (2018). Sensory Over-Responsivity: An Early Risk Factor for Anxiety and Behavioral Challenges in Young Children. Journal of Abnormal Child Psychology,47(6), 1075-1088. doi:10.1007/s10802-018-0502-y
Ah, handwriting. The source and summit of our profession, right? (Just kidding.) However, while a lot of school OT’s like to remind people, “we are not handwriting teachers,” (I agree) it also makes sense as to why OT’s are called into action when a child’s handwriting is preventing them from participating in their school day.
Where do we start? What program or method do we use? Personally, I started with what information was handed down to me on Handwriting Without Tears. I particularly like the idea of developmental teaching order that they use. I think sometimes people think, “Oh, A is the first letter of the alphabet, let’s start with A.” There are diagonal lines in A, though, and children start forming those around 4 ½ years old. So, makes sense to me to start with the straight line letters first.
In recent years, I’ve been intrigued by the Size Matters program. It was new to me and I like some of the concepts I picked up from learning about it. All this to say, which program should we use?
Journal American Journal of Occupational Therapy (SNIP score 1.121)
Article Title Curriculum-Based Handwriting Programs: A Systematic Review with Effect Sizes
4 Case series (and low-quality cohort and case control study)
5 Expert opinion without explicit critical appraisal
* This was a systematic review which included many two-group non-randomized studies. As this type of systematic review doesn’t fall into either 2A nor 3A, I chose to categorize it into a level 2B study. The evidence reviewed was higher than case studies but lower than cohort studies.
Methods
A systematic review gathered articles from January 2006-December 2015 that included curriculum-based programs and handwriting intervention for students in preschool through 5th grade.
The researchers included 13 studies total, with 10 Level II, 2 Level III and 1 Level II-III studies.
Findings
Handwriting Legibility
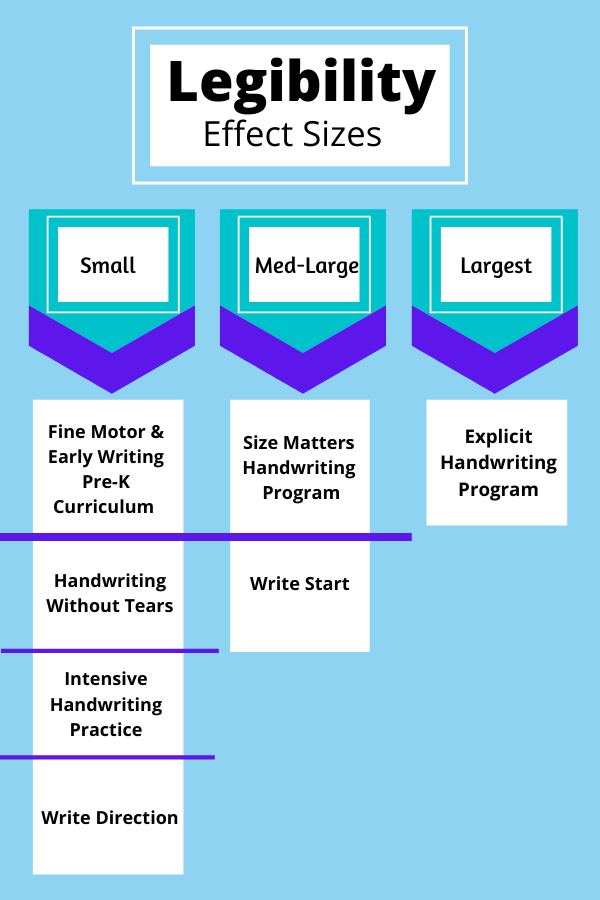
For legibility, the programs with the largest effect size was the Explicit Handwriting Program. Medium to large effects on legibility came with the Size Matters Handwriting Program and Write Start.
Programs with small or very small effect sizes on legibility included the Fine Motor and Early Writing Pre-K Curriculum, Handwriting Without Tears, Write Direction and Intensive Handwriting Practice.
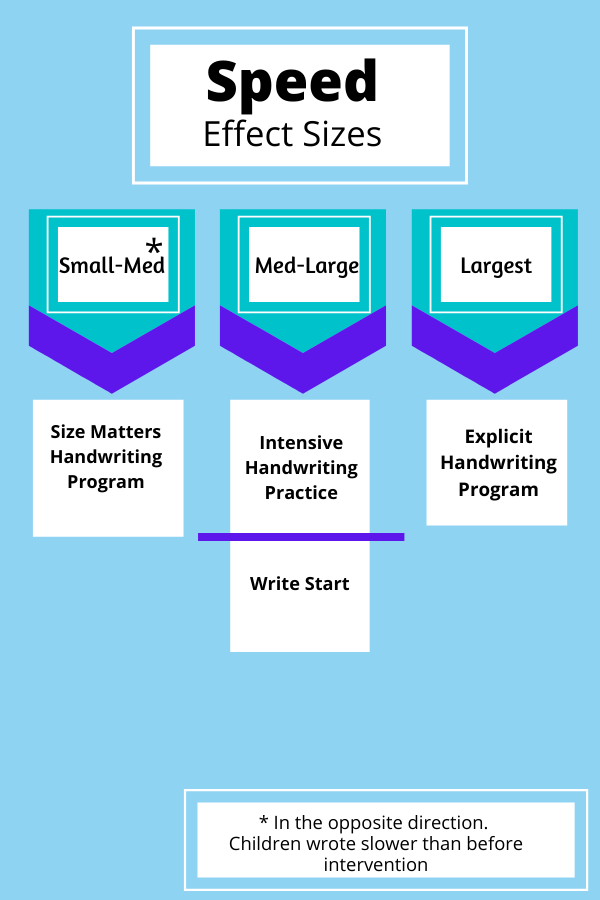
Handwriting Speed
The Explicit Handwriting Program also the largest effect sizeon speed. The Write Start and Intensive Handwriting Practice programs had small to medium effect sizes.
Size Matters Handwriting Program had small to medium effect size in the opposite direction, meaning kids wrote slower.
Fluency
Four studies assessed fluency, all investigating the Write Start program. There were significant differencesfor fluency in three of four studies. The authors noted that the studies being too similar and variations in post-test findings led them to determine there is insufficient evidence to speak to the effects of the program on fluency.
Handwriting Program Characteristics
All interventions lasted a minimum of 6 weeks, with the majority lasting more than 12 weeks. However, the total number of hours of intervention did not show a relationship with the impact on legibility and speed of writing.
The only two programs to have a larger than small effect size on both legibility and speed were the Write Start program and Explicit Handwriting Program.
Choosing a Handwriting Curriculum Based on Your Needs
An interesting highlight of this review is that different curriculums had significant effects on different outcomes. The authors suggest that OT’s consider this when choosing a curriculum to use. It may be most effective to choose a curriculum that improves legibility if that’s what you’re most concerned with.
So, the findings from this review may suggest that at this point in time, an OT may consider the following:
Legibility
The largest effect size on legibility came from students using the Explicit Handwriting Program. My initial thought was, “Okay! Let’s explore this. Seems like the best option!” Upon reading the program characteristics, it was very detailed. Intervention included dexterity exercises, discussions about context of writing with children, learning 2-3 letters in cursive per session given modeling, etc. (Kaiser, Albaret, & Doudin, 2011, p. 613, 614). That is to say, it was thorough, but is not a standardized program. The may be why the authors suggested the use of Size Matters Handwriting Program over Explicit Handwriting Program. On average, children using the Size Matters Handwriting Program and Write Start Program showed medium to large effects for improved legibility. For my part, I’m going to investigate Write Start in more detail.
Speed
From their review, the authors suggest that Explicit Handwriting Program, Write Start or Intensive Handwriting Program may be the best choices for curriculum if your primary concern is speed.
Things to Consider
The authors mention that they did not include level I studies in the review, as there were not any studies of that level of evidence that met inclusion criteria. Level I studies would give us more robust evidence to make our decisions on which program to use. The authors also mentioned that the way they measured their data on effect sizes did not take into consideration for repeated measures. They note that they intentionally did this to be conservative, but that this method may have produced effect sizes that were smaller than they really were.
What Do You Think?
What programs do you typically use with your students? Which programs mentioned here are new to you?
References
Engel, C., Lillie, K., Zurawski, S., & Travers, B. G. (2018). Curriculum-Based Handwriting Programs: A Systematic Review With Effect Sizes. American Journal of Occupational Therapy,72(3). doi:10.5014/ajot.2018.027110
Kaiser, M., Albaret, J., & Doudin, P. (2011). Efficacy of an Explicit Handwriting Program. Perceptual and Motor Skills,112(2), 610-618. doi:10.2466/11.25.pms.112.2.610-618