Parents and therapists alike may tell you picky eating seems to have grown tremendously in recent years. While there is some amount of typical toddler fussiness, sometimes picky eating is indicative of something more.
As with anything, likely there are a wide variety of factors to include in the possible explanations. Challenges with sensory processing often contribute to difficulty with feeding. Processed food has become almost a staple in families’ homes. With this we have seen a decrease in families and children planting, growing, interacting with and preparing food in its fresh and natural form. Eating dinner together as a family is a hugely important activity. Here children observe and learn what to think about food and how to eat it from those with whom they share the dinner table. While some families returned to the dinner table due to lockdowns during COVID-19, it’s a habit that is not as often prioritized into overly packed after school and work schedules.
Picking Eating, Parents and Family Dynamics
Whatever the cause of picky eating, it can greatly impact family stress levels and dynamics. I always say I have a love/hate relationship with feeding therapy. I really think it’s fun, and I love when kids make progress and grow confident to try new foods! However, moving that progress to the family dinner table can be another story. Picky eating requires treatment of the whole family. Parents in particular need to play an active role in learning how to teach their picky eaters about new foods.
That’s why I loved the article I reviewed this week. It specifically focused on educating parents and empowering them so they can be the crucial agents of change their children need them to be! This article actually covers treatment of children who had a diagnosis of Avoidant-Restrictive Food Intake Disorder (ARFID). That is not your garden variety picky eater. The Washington Post published a story last week on the topic. In the article, the author of the study I’m reviewing today shared about her experience working with children with ARFID.
Journal Cognitive and Behavioral Practice (SNIP score 0.994)
Article Title The (Extremely) Picky Eaters Clinic: A Pilot Trial of a Seven-Session Group Behavioral Intervention for Parents of Children with Avoidant/Restrictive Food Intake Disorder
- 1A Systematic review of homogeneous RCTs
- 1B Well-designed individual RCT
- 2A Systematic review of cohort studies
- 2B Individual prospective cohort study, low quality RCT, ecological studies; and two-group, non-randomized studies
- 3A Systematic review of case control studies
- 3B Individual retrospective case-control studies; one-group, non-randomized pre-post test study; cohort studies
- 4 Case series (and low-quality cohort and case control study)
- 5 Expert opinion without explicit critical appraisal
Methods
The authors trained cohorts of parents whose children presented with criteria for avoidant/restrictive food intake disorder (ARFID). Parents of 21 children, ages 4-11 years old, participated. Cohorts had two to four families each. Seven total cohorts participated, with each cohort participating in seven sessions of the manualized group treatment for parents only.
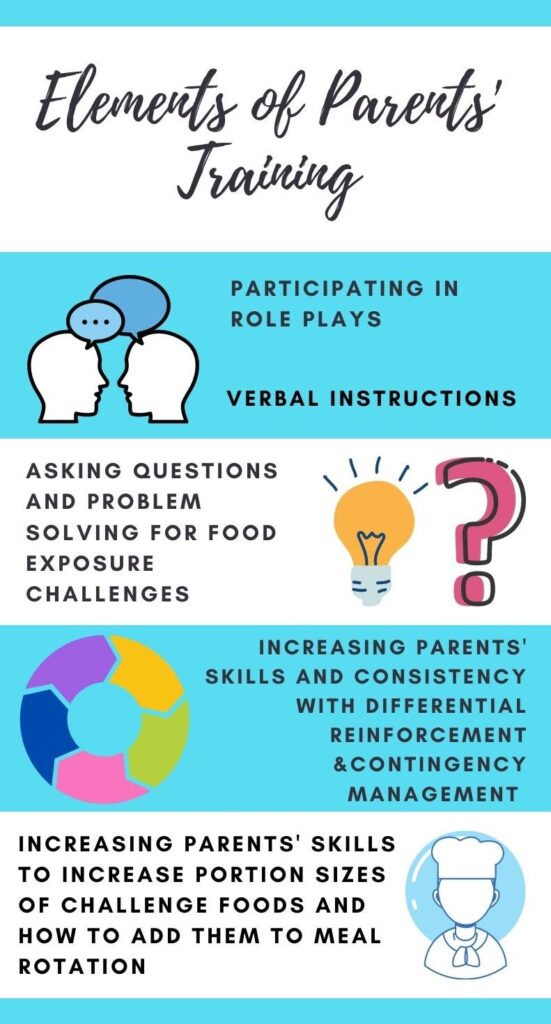
Interventionists trained the parents in acting as coaches in presenting non-preferred foods on a daily basis in their homes. They also empowered parents on how to reduce problematic mealtime behaviors with parent management training. The participants in this study were referred to a specific provider, the clinical director of an outpatient anxiety speciality clinic which serves to evaluate and treat extremely picky eating (Dahlsgaard & Bodie 2019, p. 9).
Children met inclusion criteria if they were 4-12 years old, had a diagnosis of ARFID and their parents’ main concern was their picky eating in the event of coexisting psychiatric or medical problems. All parents completed the following standardized feeding measures at pretreatment, posttreatment and a 3-month follow-up to assess their child’s picky eating and problematic mealtime behaviors (Dahlsgaard & Bodie 2019, p. 3).
- Behavioral Pediatric Feeding Assessment Scale
- Child Eating Behaviors Questionnaire
Parents completed the Child Behavior Checklist during intake only as a means of collecting information on behavioral, emotional and social problems (Dahlsgaard & Bodie 2019, p. 12).
Intervention
Parents participated in seven 90 minute sessions which occurred weekly for sessions 1-4. The last two sessions occurred with a 3-4 week gap to promote families practicing the skills they had learned (Dahlsgaard & Bodie 2019, p. 14). The seventh session was an optional follow up. Interventionists educated parents on ARFID, mealtime hygiene, appetite optimization and the key behavioral principles for the program in the first session (Dahlsgaard & Bodie 2019, p. 14).
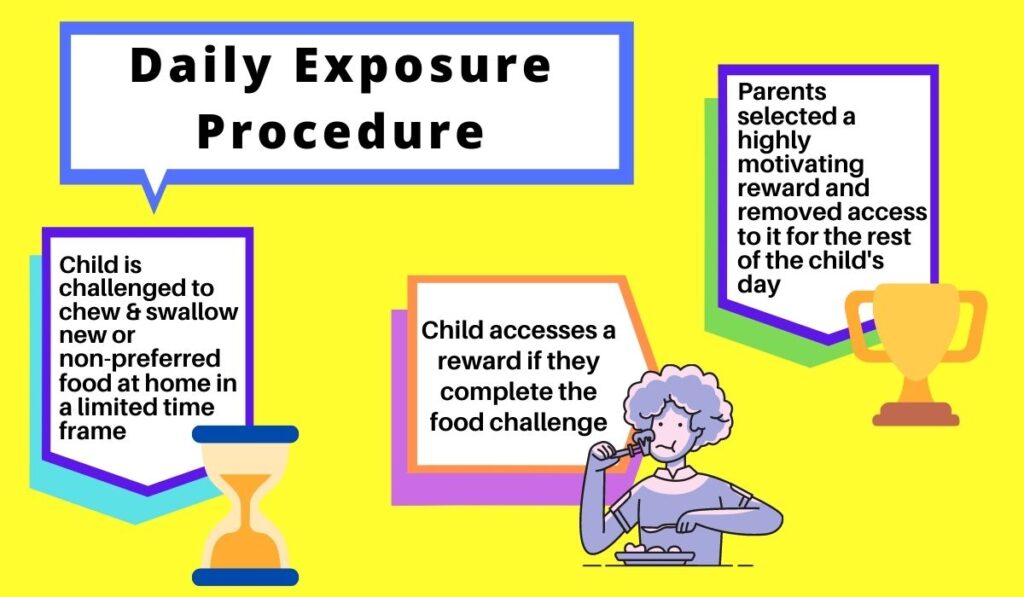
Interventionists taught parents how to implement daily exposure procedures in the second session. Following sessions focused on improving parents’ ability to follow through with promoting appropriate responses to children’s behaviors as well as implementing contingency management for food exposures and meals. Parents also learned about increasing the size of challenge food portions and incorporating them into meals.
Findings
Behavioral Pediatric Feeding Assessment Scale
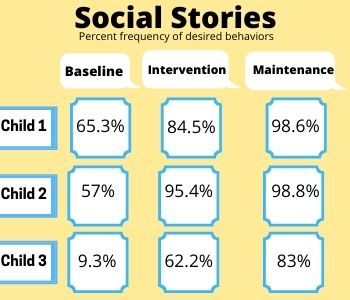
Significant reductions were reported for all four subscales of this assessment along with a large within-group effect size at posttreatment (Dahlsgaard & Bodie 2019, p. 16). At the 3-month follow-up, gains were maintained and the large within-group effect size remained.
Child Eating Behaviors Questionnaire
Parents ratings on the CEBQ demonstrated a significant increase for Enjoyment of Food as well as significant decreases for Slowness in Eating, Satiety Responsiveness and Food Fussiness from pre to post treatement (Dahlsgaard & Bodie 2019, p. 16). The author noted large within-group effect sizes in these areas at posttreatment.
No significant improvements were observed for Emotional Undereating on this assessment. Enjoyment of Food resulted with a significant increase from pre-treatment to the 3-month follow up, and significant decreases for Satiety Responsiveness, Slowness in Eating, Emotional Undereating and Food Fussiness. The author reported moderate-large within-group effect sizes. All of these gains remained at the 3-month follow up.
Parent Satisfaction
Of the parents who completed treatment satisfaction questionnaires post-treatment (71% of the total study participants) 96% of those parents rated specific elements of the Picky Eaters Clinic as Very Helpful or Extremely Helpful (Dahlsgaard & Bodie 2019, p. 17). Parents reported the support they received from the group and trainings in food exposures as well as contingency management as the most helpful elements (Dahlsgaard & Bodie 2019, p. 17).
Things to Consider
The parents in this study were highly motivated as demonstrated by 95% attendance rate and 71% of children having two parents attending treatment sessions (Dahlsgaard & Bodie 2019, p. 15). This study’s author noted that this group was fairly heterogeneous, but that previous research indicates that this is consistent for children with a picky eating subtype diagnosis of ARFID (Dahlsgaard & Bodie 2019, p. 27).
Interestingly, there are three subtypes of ARFID. These include those children with extreme picky eating, but also children whose avoidance of eating stems from a specific fear/potential negative consequences they they associate with eating. This can include things like a phobia of choking, having allergic reactions or vomiting. A third group of children who fall into the ARFID category are those who demonstrate decreased interest in eating.
This information is relevant as the treatment one selects varies depending on the subtype the child presents with. It is important to be specific and intentional with our selections of evidence based treatments to promote progress for children and their families!
The author also mentions that the data that was used was obtained in clinical procedure as opposed to following a research protocol. She noted that this type of data is often less reliable and complete (Dahlsgaard & Bodie 2019, p. 27). Finally, as there was no control group for this study, we can not compare it to the effectiveness of other common treatments for selective eating.
The More You Know…
So now that you know that involving parents only resulted in significant changes in the relationship with food for children with Avoidant-Restrictive Food Intake Disorder (ARFID), how do you plan to educate and empower parents of the children you’re treating? I highly recommend this article on How to Get Picky Eaters to Try New Foods as a starting point!
References
Dahlsgaard, K. K. & Bodie, J. (2019). The (extremely) picky eaters clinic: A pilot trial of a seven-session group behavioral intervention for parents of children with avoidant/restrictive food intake disorder. Cognitive and Behavioral Practice, 26 (3), 492-505. https://doi.org/10.1016/j.cbpra.2018.11.001