Sensory processing is so central to what peds OT’s do these days, but there remains a lot of difference in opinions. From “whether it exists,” to what’s the most effective way to treat it. One often leaves OT school feeling like there’s still a lot of new learning to be done.
Learning curves for new grads can be steep. I will say that I personally have shifted my thinking dramatically as an OT since the time I graduated. I have gone from being verydetail oriented, goal focused, everything must look like typical to much more practical, holistic and functional.
This journey has led me to be interested in developmental approaches like the DIR/Floortime model. From what I’ve read, it is a collaborative approach between parents and professionals, in which parents are key players. It also emphasizes emotional development and engagement. These are also two elements that have become largely more important to me as I’ve learned to see the forest instead of focusing only on the trees.
I plan to research more into DIR and similar approaches, but this was a basic starting point on an article that reviewed DIR’s impact on communication and self-regulation.
Journal Journal of Occupational Therapy, Schools, & Early Intervention (SNIP 0.535)
Article Title Intervention effects on communication skills and sensory regulation on children with ASD
4 Case series (and low-quality cohort and case control study)
5 Expert opinion without explicit critical appraisal
Methods Professionals recruited 25 children aged 3-6 years old with ASD and their families to participate in this study.
Intervention
A multi-disciplinary team developed focused individualized intervention plans for each child that were completed for a 10 month period. The programs included 1-2 elements that were included in the approach: Floortime, sensory integration and speech therapy (Helena I. S. Reis, Ana P. S. Pereira & Leandro S. Almeida p. 349, 2018). Important aspects of the intervention process included:
A team of multi-disciplinary professionals who worked as a team with families
Identifying children’s strengths, preferences and interests
Focusing on developmental areas that emphasis connection, engagement and social skills to promote learning in a child’s natural environments
Every member of the team of professionals was trained in DIR/Floortime and OT’s additionally were trained in Ayres Sensory Integration (Helena I. S. Reis, Ana P. S. Pereira & Leandro S. Almeida p. 350, 2018). All team members had also worked for more than 5 years in the Early Intervention System with children with ASD.
Sessions were as follows…
Floortime A psychologist led parents in 30 minute Floortime sessions, in which psychologists coached parents in promoting joint attention from their child. The psychologist also observed and provided feedback to the parent utilizing these skills following the time spent working together.
Sensory Integration OT’s led sessions for 30 minutes if the child participated in multiple therapies from the three options (SI, Floortime and Speech therapy). The children who only participated in SI therapy participated in 45 minute sessions. OT sessions aimed to promote joint attention, social skills, perceptual skills and motor planning through eliciting increased integration of sensory input.
OT’s also provided education to parents as to the connection between sensory integration abilities and difficult behaviors children sometimes display. In this education, OT’s included information on how to adapt the child’s every day routine with modifications to promote regulation.
Speech Therapy Speech therapists used augmentative and alternative communication systems in sessions to promote natural gestures and symbolic communicative forms during their 30 minute sessions (Helena I. S. Reis, Ana P. S. Pereira & Leandro S. Almeida p. 352, 2018).
Measures Parents completed the Assessment Scale of Children with ASD, which gathers information on Social Communication, Repetitive Behaviors and Restricted Interests, and Sensory Processing.
Findings
Children demonstrated statistically significant improved scores for the areas of Social Communication and Sensory Processing. The area of Repetitive Behaviors and Restricted Interests did not yield a statistically significant in the change in parents’ ratings.
Things to Consider
The authors note that the study had no control group, so the results cannot be compared to a lack of treatment, alternative treatment, nor control for development by maturation alone. They also noted that they did not compare or categorize children based upon the severity of their symptoms of each area included.
A limiting element in applying this study to a wide array of OT’s is that the OT’s in this study were trained in both Ayres Sensory Integration and Floortime. I definitely believe I do Sensory Integration Therapy based on the principles in the infographic above, but I’m not officially trained. What I do take away from this article is evidence that developmental models such as DIR/Floortime are a valuable tool to enhance the occupational therapy one is already providing.
References
Helena I. S. Reis, Ana P. S. Pereira & Leandro S. Almeida (2018). Intervention effects on communication skills and sensory regulation on children with ASD, Journal of Occupational Therapy, Schools, & Early Intervention, 11:3, 346-359, DOI: 10.1080/19411243.2018.1455552
Watling, R., & Hauer, S. (2015). Effectiveness of Ayres Sensory Integration® and sensory-based interventions for people with autism spectrum disorder: A systematic review. American Journal of Occupational Therapy, 69, 6905180030.
4 Case series (and low quality cohort and case control study)
5 Expert opinion without explicit critical appraisal
* This was a systematic review which included mostly RCT’s and Level II studies. As this type of systematic review doesn’t fall into either 1A nor 2B, I chose to categorize it into a level 2A study. The evidence reviewed was higher than case studies but lower than cohort studies.
Methods
The authors of this systematic review included studies that investigated the effect of interventions that are not Ayres Sensory Integration specifically. They included studies published between 2007 and May 2015. Authors included studies on sensory-based techniques as well as sensory environmental modifications. Interventions targeted clients between 2-21 years old with sensory integration difficulties. Authors ensured that articles investigated specific sensory techniques or sensory environmental modifications.
Findings
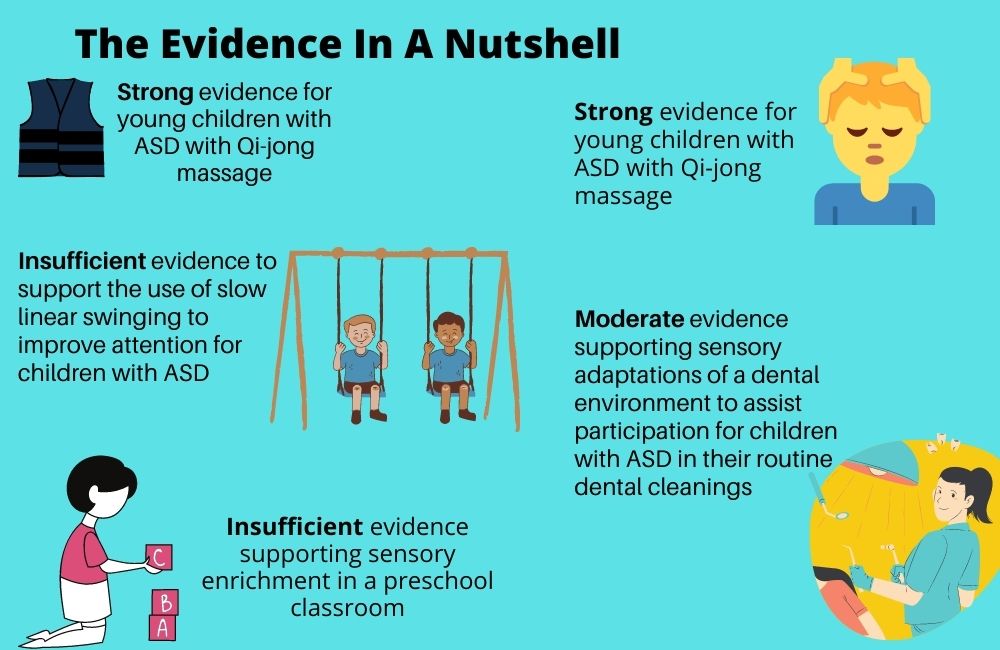
Qi-jong massage The authors concluded there is strong evidence for young children with ASD with Qi-jong massage (Bodison, S.C. & Parham, L.D. 2017, p. 5).
Three Level I and and 1 Level II studies demonstrated improvements in self-regulation, parenting stress, tactile differences and ASD symptoms. Children were 2-7 years old and had ASD. Their parents, after being trained by occupational therapists, provided 15 minute daily massage. The studies lasted 4 and 5 months.
Important to note is that the OT’s had at least 50 hours of training in Qi-jong before training parents on its implementation. This may make it a challenge intervention for most OT’s to implement.
Weighted Vests The authors concluded there is limited evidence for the use of weighted vests for children with ADHD (Bodison, S.C. & Parham, L.D. 2017, p. 5).
A level I study did show improved attention and in-seat behavior when a group of 6-9 year olds wore vests with 10% of their body weight. The authors mention that limitations in the design of the study impacted its internal validity. This in turn caused them to interpret these findings with caution.
Study authors also noted that the evidence they found for the use of weighted vests with children with ASD had low levels of evidence, so these studies were not formally included in the review. The authors conclude the evidence for the effectiveness of weighted vests for children with ASD is insufficient at this time.
Slow Linear Swinging The authors concluded there is insufficient evidence to support the use of slow linear swinging to improve attention for children with ASD.
A level I study investigated the impact of being on-task following slow, linear swinging in a group of children with ASD. The study demonstrated no significant difference between children who swung and those in the control group (Bodison, S.C. & Parham, L.D. 2017, p. 6).
Study authors did note a limitation of this study is that the arousal level of children was not assessed prior to their participation in swinging. They posited, therefore, that if a child was in a low arousal state prior to a calming activity, this may have demonstrated no positive impact on the child’s on-task behaviors.
Sensory Enrichment in Preschool The authors concluded there is insufficient evidence supporting sensory enrichment in a preschool classroom.
This level I study investigated the impact of embedding tactile, proprioceptive and vestibular activities for 12 weeks in a preschool classroom’s daily routine. All children in the classroom participated in these activities, but one group of children also received ASI through OT sessions.
Both groups improved in their play skills, but no difference was noted between them. Study authors of this review mention that design limitations, including a very small sample size of 8, limit the implications of the study findings.
Sensory Environmental Modifications The authors concluded there is moderate evidence supporting sensory adaptations of a dental environment to assist participation for children with ASD in their routine dental cleanings (Bodison, S.C. & Parham, L.D. 2017, p. 6).
Children reported improved measures of pain intensity and sensory discomfort as well as improved participation in dental cleaning for typically developing children and those with ASD. Children received deep pressure from a decorative wrap and the auditory and visual aspects of the the dental environment (Bodison, S.C. & Parham, L.D. 2017, p. 7).
Most interesting to me is that investigators measured children’s electrodermal responses as a means to quantify impact on stress and anxiety. They found a moderate to large effect size for children with ASD after they received the intervention!
So What Do You Think?
I appreciate when studies have high standards for the research they include in their reviews. However, due to the nature of the current evidence in OT, that sometimes means there is limited information on the interventions we use most.
I’m interested in the idea of Qi-jong massage, but I will say that the skeptic in me thinks, “Well, if anyone received a 15 minute massage to start their day, I would definitely expect them to show improvements in their behaviors.” I also am curious to see if the massage was compared to other interventions such as a tailored sensory diet. If families really followed up with those every day with good fidelity, I hypothesize that we would similarly see as good if not better results in the developmental gains for children.
Reference
Bodison, S.C., and Parham, L.D. (2017). Specific Sensory Techniques and Sensory Environmental Modifications for Children and Youth with Sensory Integration Difficulties: A Systematic Review. American Journal of Occupational Therapy72 (1). https://doi.org/10.5014/ajot.2018.029413
“You’re the physical therapist, right?” “Oh, here comes the handwriting teacher.” “Can you get me a weighted vest for him? He can’t sit still.”
All school based OT’s have heard one of these statements at some point in their career. While it sometimes takes a couple of years for teachers to recognize and understand who you are and what your role is, I love school OT. It is my jam. What appealed to me most about the school setting as a new grad was built in teammates. I was blessed with an enthusiastic and encouraging special education teacher. She planted the first seeds of teaching me to appreciate small gains and to realize I can’t control everything.
Backing Up Our Recommendations with Evidence
So what does the evidence say about the interventions OT’s use and the ones that many of our coworkers request? This systematic review will give you insight to just that–stability balls, handwriting interventions and weighted vests, to name a few favorites. Check it out below and see what areas you may want to reassess in your own practice.
Journal American Journal of Occupational Therapy (SNIP score 1.121)
Article Title Interventions Within the Scope of Occupational Therapy to Improve Children’s Academic Participation: A Systematic Review
4 Case series (and low quality cohort and case control study)
5 Expert opinion without explicit critical appraisal
* This was a systematic review which included a wide array of evidence from RCT to Level III studies. As this type of systematic review doesn’t fall into either 2A nor 3A, I chose to categorize it into a level 2B study. The evidence reviewed was higher than case studies but lower than cohort studies.
Methods
The authors of this systematic review included studies that were peer-reviewed, in English and published between January 2000 through March 2017. They included only level I-III studies that fell within the scope of occupational therapy. Although many studies were not completed by OT’s, the authors did require that school practitioners or researchers conducted the studies. The study authors grouped articles into three categories:
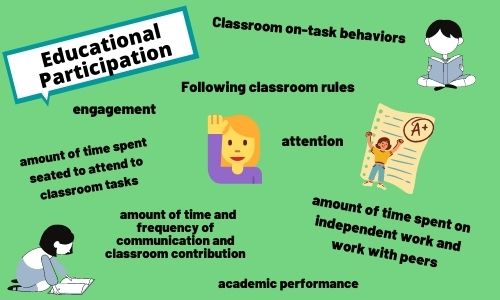
Educational Participation
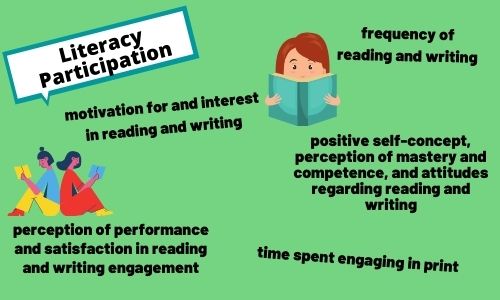
Literacy Participation
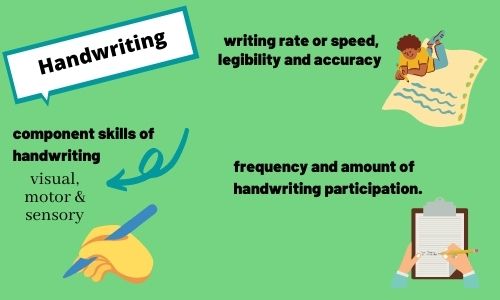
Handwriting
Findings
Educational Participation
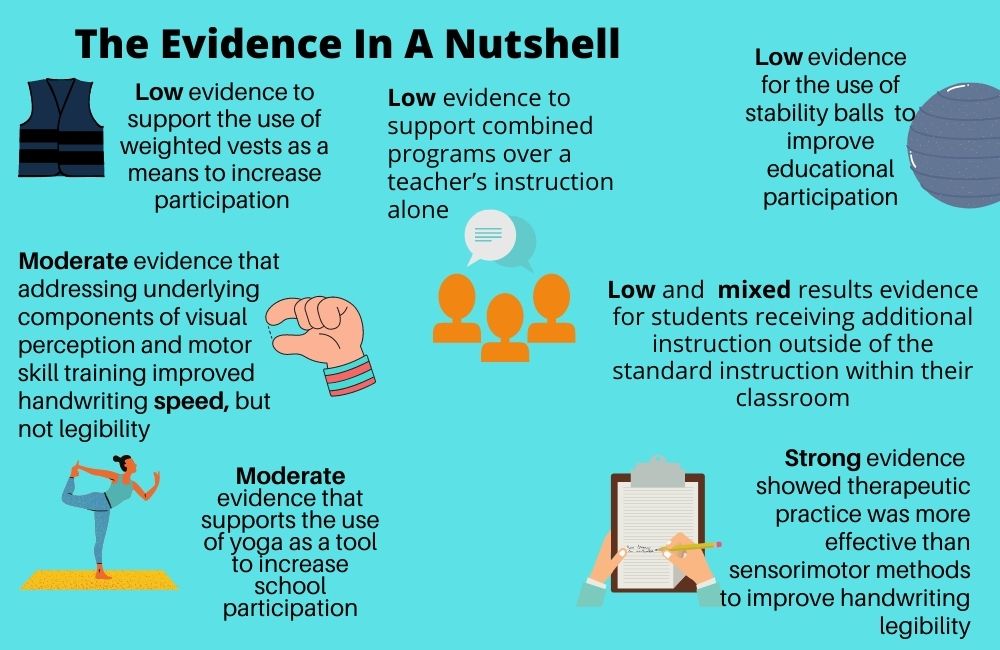
Weighted Vests The authors of the review concluded there islow evidence to support the use of weighted vests as a means to increase participation as from the evidence below.
In a Level II study, students with ASD served as their own controls in three conditions when they did not wear a vest, wore a vest with weight and wore a vest without weight. The targeted outcomes of time sitting, attention to task and seated behavior did not significantly improve.
The Evidence Points Toward…Insufficient Data to Say
A systematic review investigated 13 studies that were group or single-case studies with children with ASD. Eight studies indicated weighted vests are an ineffective tool to increase seated behaviors and engagement. Five studies did show strong support. Small sample sizes and a limited geographic area represented in the samples limit the external validity.
Stability Balls The authors of the review concluded that there is low evidence for the use of stability balls to improve educational participation.
In an RCT in a gen ed second grade classroom, students who sat on standard chairs were on task more often when working with peers and independently than those seated on stability balls.
In a level III study, investigators observed students in a second-grade classroom while using standard classroom chairs and then twice using stability balls. They found a significant increase in students being on task while the students used stability balls.
A second level III study found eight students with ADHD in 3rd-5th grade showed a significant increase in the average time they remained in their seat and the time they spent on task.
Yoga Authors of this systematic review concluded there is moderate evidence that supports the use of yoga as a tool to increase school participation.
A level III study assessed the Yoga4 Classroom program for second grade students and showed significantly increased attention and on-task for academic tasks.
Students in the intervention group of an RCT for a manualized yoga program geared toward social-emotional wellness in sixth to ninth graders showed significantly higher levels of school engagement than the control group.
A systematic review found children with learning disabilities, emotional and behavioral problems showed significant improvements in their communication and classroom contribution compared to control groups. However, the authors deemed the evidence inconclusive due to a high risk of bias.
Literary Participation
Full disclosure-I’ve excluded some findings in my reporting. Not to skew the findings, but to include the elements that seem most realistic for an OT to include in their session.
Strong evidence from four studies showed that children who participated in embedded creative and engaging literacy activities in small groups had significant increases in their positive attitude toward reading. They also showed an improved self-concept as a reader. An intervention mentioned that OT’s could definitely include is to have students create a story with the use of drawings and interactive discussions (Grajo, Candler, & Sarafian, 2020, page 6).
Handwriting The authors broke down the data on handwriting interventions into the domains listed in the headings below
Approaches to Address Component Skills
Authors reviewed four RCT’s to determine how addressing the underlying components of motor skills, kinesthesia and visual perception impact legibility. The study on kinesthesia did not demonstrate improvement. The remaining RCT’s showed moderate evidence that addressing underlying components of visual perception and motor skill training improved handwriting speed. These methods did not impact handwriting legibility.
Sensorimotor vs. Therapeutic Practice
Seven studies investigated the difference between sensorimotor activities and therapeutic practice.
Sensorimotor activities addressed visual perception, kinesthesia, visual-motor integration, in-hand manipulation, and the biomechanical features of handwriting. Therapeutic practice included paper and pencil activities that implement cognitive aspects of feedback on the child’s performance as well as self-evaluation (Grajo, Candler, & Sarafian, 2020, page 8).
Strong evidence from 1 Level II and 3 Level I studies showed therapeutic practice was more effective than sensorimotor methods to improve handwriting legibility for children with handwriting challenges,.
Interventions in Addition to Usual Classroom Activities
The evidence for students receiving additional instruction outside of the standard instruction within their classroom was low and with mixed results. An RCT and Level II study found for typically developing children there was a significant positive result with the use of additional instruction. Two different studies assessed differences between children receiving additional intervention and those who did not. These studies did not yield a significant difference between the groups’ performance.
Interventions in Place of Usual Classroom Activities
The review found results from six studies (4 Level II and 2 Level III) that combined programs (often the teacher and an OT working together to teach handwriting) has low evidence to support these over a teacher’s instruction alone. Of note is that there were insufficient details provided on the “typical classroom curriculum” that these combined programs replaced. Thus, one is limited in drawing a conclusion on the effectiveness of combined programs over a standard classroom curriculum.
A Level II study compared a manualized combined program to a manualized program of therapeutic practice found no differences between the two. Finally, a Level II study found a teacher’s designed instruction was more effective than a combined program that was manualized.
Of Note
The authors mention that limitations of this systematic review include some studies having no control group nor random sampling in addition to small sample sizes. They also included that many studies were completed by practitioners outside of occupational therapy, such as school psychologists, reading interventionists, etc. However, the interventions were within the scope of OT practice. Therefore, they suggest that one may be limited in the ability to predict how these interventions and findings would generalize to pediatric OT’s practicing in schools and clinics.
What did you learn?
For me, it is always a little disheartening to read evidence that does not support sensorimotor approaches over therapeutic practice. Sensorimotor is fun and engaging, and I do believe children are learning when we teach them this way! However, if the evidence is pointing toward therapeutic practice to be more effective to improve legibility for handwriting, I think we have a duty to accept that and incorporate these strategies into our sessions.
By no means do I think we can’t use something if there is not an article to back it up. However, I think we need to consider the evidence and make sure evidence based treatments are taking up the majority of our treatment time!
References
Grajo, L. C., Candler, C., & Sarafian, A. (2020). Interventions Within the Scope of Occupational Therapy to Improve Children’s Academic Participation: A Systematic Review. American Journal of Occupational Therapy,74(2). doi:10.5014/ajot.2020.039016
Telehealth has drastically changed the way many therapists are practicing in these past six months. (Six months! Can you believe that?) I haven’t personally tried my hand at it because I was let go from my job when COVID closed schools and clinics in March. I am always eager to hear my former coworkers talk about their experiences navigating the unchartered waters of telehealth. I’ve also admired the creativity, ambition and flexibility as I see resources, tips and tricks that therapists new to telehealth have discovered and shared.
Adapting to Telehealth Like Champs
I may be biased, but therapists are incredible people. While the adaptability, creativity, goal setting and executing that many bring to the field has made providing telehealth services possible, I have to believe many are grieving the loss of in person therapy. I’m getting married and moving abroad in a month or so, so it didn’t feel like the right timing for me to get a new job. However, I have thought about how I hope to get an OT job when I move. I’ve had to tell myself that I might have to be open to telehealth if that is what my option ends up being, and that makes me so sad.
But, alas, accept the current state of society we must. My goal in covering this topic is to encourage people doing telehealth that what you’re doing can make a difference! I know I’ve heard many people say, “It’s not really effective.” I can certainly imagine that, if the parents aren’t involved. There are often factors we can’t control. However, there are always things that are within our power to change.
How to Provide Effective Telehealth OT Services
I’m hoping this article review serves as encouragement that doing the hard work to shift our thinking even more from “I’m the therapist and I’ll make the change,” to “We’re working as a team and my collaborating with the caregivers will help this child to continue to succeed,” is worth it. You will also find some specifics and direction of elements that the investigators in this study used in order to promote successful parent coaching.
JournalThe American Journal of Occupational Therapy (SNIP score 1.121)
Article Title Occupation-Based Coaching by Means of Telehealth for Families of Young Children with Autism Spectrum Disorder
Authors Lauren M. Little, Ellen Pope, Anna Wallisch, Winnie Dunn
4 Case series (and low-quality cohort and case control study)
5 Expert opinion without explicit critical appraisal
Methods
The study investigators recruited children in underserved and rural areas through early intervention and early childhood programs. Investigators included children with an Autism Spectrum Disorder who were 0-6 years old. Seventeen families completed the intervention.
Intervention
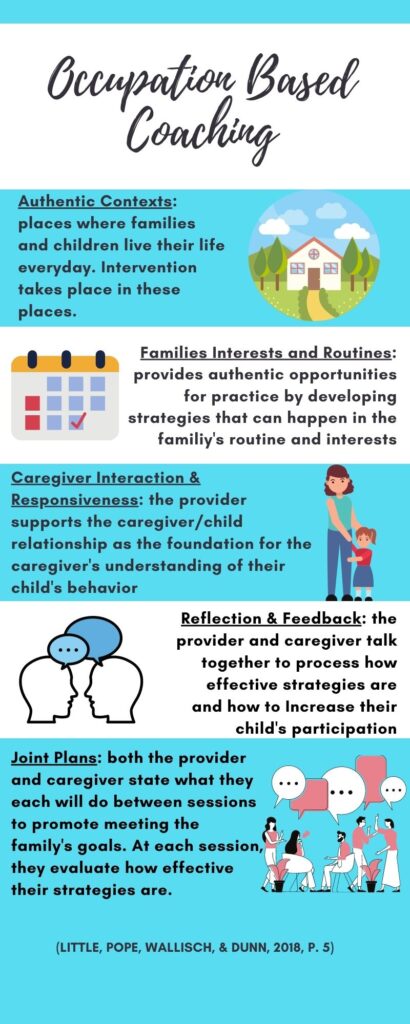
Occupational therapists completed 12 weeks of coaching sessions through Zoom. Therapists used the coaching model to empower families to understand and grow confident in the knowledge they have in regards to their child. The therapists ask questions to promote reflection, guide families to realize what knowledge they already have and use, as well as to guide families in developing and implementing strategies to assist their children in meeting goals the family set.
OT’s used the first session to complete a routine-based questionnaire as a means to gather information on the family’s daily routines and context of their daily activities. The family then came up with goals for the OT sessions. Investigators used the following measures to gather relevant data for the intervention.
Demographic Form-Family
Sensory Profile-Second Edition
Social Responsiveness Scale-Second Edition
Parenting Sense of Competence Scale
Assessment of Preschool Children’s Participation
Canadian Occupational Performance Measure-Second Edition
Study authors also used Goal Attainment Scaling to work with parents in establishing goals. This is a documentation method that uses established, sensitive levels of change for a targeted goal to demonstrate progress in that area.
Findings
Authors compared the mean scores of each measure from pre and post intervention to determine the effects of intervention.
Parent Efficacy as a Result of Telehealth Coaching
Post-intervention scores for the Parenting Sense of Competence Scale (PSOC) demonstrated a significant increase in parents’ feelings of efficacy. This indicates that parents felt more equipped and able to manage the situations they encounter as a parent. Parents did not report increased levels of satisfaction. Satisfaction included the degree to which a parent reports their role as a parent is comfortable and rewarding (Little, Pope, Wallisch, & Dunn, 2018, p. 4)
(Little, Pope, Wallisch, & Dunn, 2018, p. 4)
Child Participation as a Result of Telehealth Coaching
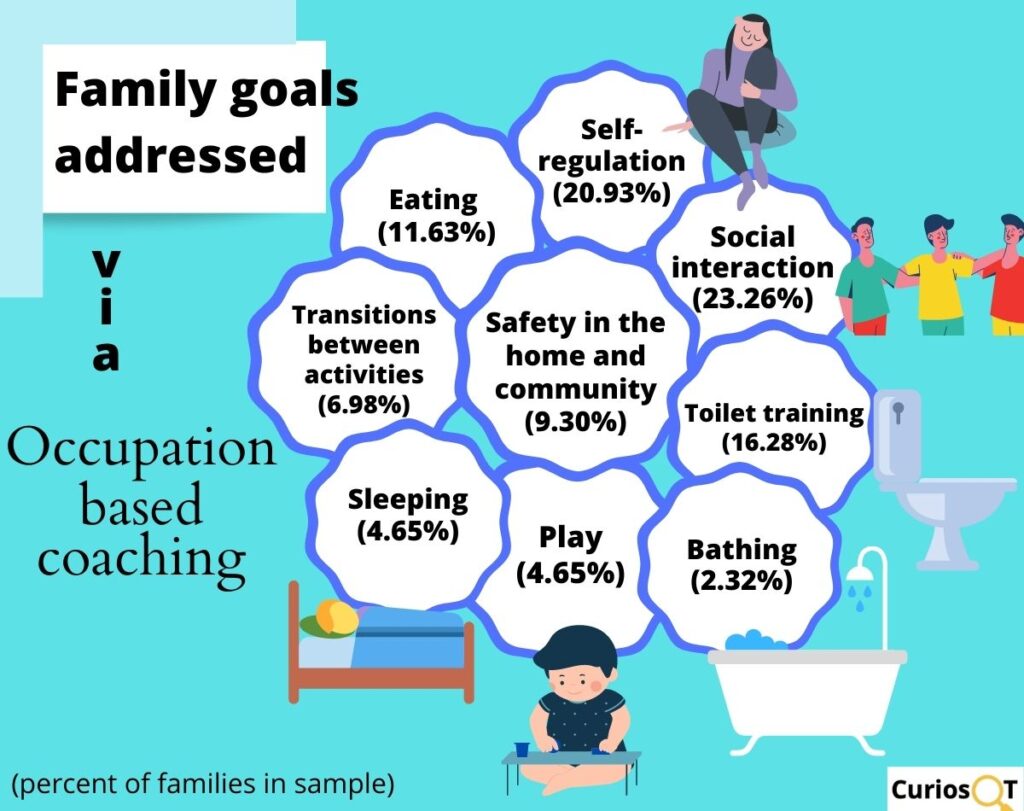
The authors measured child participation with the Assessment of Preschool Children’s Participation (APCP), GAS goals and COPM-2. The frequency with which children participated in activities and the diversity of the activities in which children engaged significantly increased per the APCP. There was also a significant increase in parents engaging in more play activities with their children as well as trying a wider variety of activities to develop their child’s skills (Little, Pope, Wallisch, & Dunn, 2018, p. 5).
Children’s increased participation in activities was significant per data from the COPM-2. Parents’ satisfaction with intervention goals increased significantly, and children made significant gains in their GAS goals.
Things to Consider
The study authors mention that only parent report measures were used to gauge effectiveness of the intervention. They suggested that the addition of objective measures of behavior or performance may enhance understanding of coaching on child performance outcomes. They also mentioned that the use of a control group may be helpful to further understand the effectiveness of telehealth vs. other modes of service or no intervention. Finally, the need for a larger sample size was mentioned.
Experiences of Parents of Children with ASD to Guide Telehealth Intervention for Others
While the current study included only parents of children with ASD, I think this information serves as a good guide for coaching a wide variety of parents. A factor that is relevant to me is that these families lived in rural or underserved areas. There may be cultural differences for families with whom we are working who are receiving telehealth services due primarily to COVID. Most notably, I think of families in suburban or urban areas that may fill their schedules more than what I often see as a slower pace of life in rural areas. However, the fact that families were able to effectively use technology to participate at a distance and make significant measurable change is encouraging.
How is your experience with telehealth going?
Have you had to switch to providing telehealth this past year? What tools and resources are you finding helpful?
References
Little, L. M., Pope, E., Wallisch, A., & Dunn, W. (2018). Occupation-Based Coaching by Means of Telehealth for Families of Young Children With Autism Spectrum Disorder. American Journal of Occupational Therapy,72(2). doi:10.5014/ajot.2018.024786
Case series (and low-quality cohort and case control study)
Expert opinion without explicit critical appraisal
Play as Occupation
Play is the quintessential occupation of all children. It impacts self-regulation, problem solving, confidence, emotional well being, creativity and more. In our ridiculously overscheduled culture, play is losing its footing and child development specialists are strongly advocating for people to comprehend and believe its worth. Play is fundamentally crucial right now as children live in a season of history with significant change to routines and dynamics. We are addressing important social issues, and throughout this children need time to play to help their emotional and mental health.
Uncovering the Skills That are Already There
Children with an Autism Spectrum Disorder have a different approach to many domains of life, including play. I personally believe that there is great value in children playing in a way that is naturally motivating, interesting and rewarding to them. However, I also believe that scaffolding and expanding the play skills of children with ASD is extremely beneficial. Improving play skills can lead to improved problem solving, perspective taking, relationships, communication skills and more. Meeting the child at their interests and style of play while emphasizing connection and relationship building both respects who they are while also seeking to provide them with an increased range of life skills.
More Play is Better for Everyone!
Also, let’s not forget how important it is for parents, siblings and friends to be able to meaningfully connect with their loved ones who have ASD. The child who expands his or her play skills is not the only person who benefits from their increased engagement in the world around them.
So how do we go about promoting an increase in play skills for kids with an ASD?
Many children on the Autism Spectrum often seek out play that is driven by the enjoyment derived by sensory stimulation. In the clinic I have loved seeing my kids with ASD grow their play skills. What most especially brings me joy is seeing them look at me in anticipation of me doing something silly or animated and then their laughter and joy that explodes when I deliver. I also love seeing what ideas they come up with and how they try to engage me in their play scheme. I have had a lot of success in using cause and effect play with balls, blocks, cars, and figurines. We often hit a stumbling block when it comes to symbolic play.
It’s Not “Just Play.”
I took the course, Play with a Purpose: Effective Play-Based Therapy & Early Child Development by Cari Ebert, and it was a game changer for me. It totally changed how I thought about therapy. I am purposeful, intentional and focused when it comes to getting things done in therapy. Sometimes I miss the forest for the trees. Learning about the development of play and how it impacts everything in a child’s development helped me to take a step back and fall in love with play. Parents often come to us wanting to address handwriting, shoe tying and meltdowns. All of those are occupations that I love. However, I came to see that if we neglect play, we are seriously limiting the progress we can help our kids to make in all other areas.
Methods
Participants
Researchers recruited caregivers and 86 children with an Autism Spectrum Disorder aged 22-36 months who attended an early intervention program. The children attended the program for 30 hours per week, during which they received behavioral, speech and occupational therapy. The researchers randomly assigned children and their caregiver to receive 10 weeks of either hands-on parent training in the JASPER program or a psychoeducational intervention (PEI).
JASPER promotes joint attention, symbolic play, engagement and regulation through a naturalistic approach. The PEI provides parents individual education and support on having children with an Autism Spectrum Disorder.
Intervention
Parents in the PEI group spent 1 hour with an interventionist per week. They learned about Autism, details of specific behavioral impairments, principles of managing behavior, strategies for teaching new skills, improving social interaction and communication, service availability, managing parent stress, and sibling/family and community responses to Autism.
A trained interventionist instructed parents in the JASPER group in 2 thirty minute sessions per week. Parents learned through a hands on approach the strategies of the JASPER method. Parents learned to identify their child’s developmental level of play as well as the child’s demonstration of social communication gestures. Interventionists taught parents to use strategies in a structured sequence in order to promote opportunities for their child to initiate interest in an activity or a toy. Parents also used these skills to promote joint attention in their play interactions with their children.
Measures
Play & Joint Attention with Parents
Examiners who were blind to the interventions coded interactions between children and parents by watching 10 minute video recordings of play sessions. This occurred pretreatment, posttreatment and 6 months after the study ended. During the sessions, researchers gave parents a standard set of toys (dolls, dishes, puzzles, trucks, shape sorter and blocks) (Kasari, Gulsrud, Paparella, Hellemann, & Berry, 2015, p. 556). Parents engaged in free play with their child using these toys. Raters qualified engagement as joint engagement if the child was aware of the parent’s participation, acknowledged their parent with non-verbal language and/or used language or demonstrated following their parent’s language in play (Kasari, Gulsrud, Paparella, Hellemann, & Berry, 2015, p. 556).
Evaluators also coded observed instances of children’s play levels, diversity of their play and instances of initiating joint attention.
Parent Stress, Language Assessment & Joint Attention with Teacher
In addition, researchers coded play interactions between children and their teacher playing together in the classroom, assessing for time spent in joint engagement. This occurred pretreatment and at the end of treatment.
Examiners used the Mullen Scales of Early Learning and Reynell Developmental Language Scales to assess receptive and expressive language skills. These items were completed pretreatment and at the follow up 6 months after intervention ended.
Parents completed the Parenting Stress Index pre-treatment, post-treatment and at the 6 month follow up, providing information about parent stress levels.
Meat and Potatoes
Duration of Joint Attention
The data analysis demonstrated a significant increase in time spent in joint engagement for the children in the JASPER group compared to the PEI group. The children in the JASPER group’s length of time jointly engaging increased by more than double. At the six month follow up, children in the JASPER group continued to have significantly higher amounts of time spent in joint engagement than peers in the PEI group (Kasari, Gulsrud, Paparella, Hellemann, & Berry 2015, p. 558).
Initiating Joint Attention
No difference by treatment group existed in impacting the rate at which children initiated joint attention. So many children demonstrated such low incidences of initiation of joint attention that they did not fall within the measurable range at baseline. Taking data from the entire sample of study participants, the mean number of children initiating joint attention increased and the total number of children demonstrating initiation of joint attention increased significantly over the six months. It did not differ by group.
Functional Play Types
Children in the JASPER group demonstrated statistically significant higher types of functional play than the children in the PEI group. At the time of the 6 month follow up, the difference between the incidences of functional play between groups was not significant.
Symbolic Play Types
The group to which children belonged had no statistically significant impact on the occurrences of symbolic play or the rate at which children increased their symbolic play skills. This remained consistent at the 6 month follow up.
Highest Play Level Achieved
Children in the JASPER group increased more in achieving higher levels of play than their peers in the PEI group. However, at 6 months, the difference between the achievement of highest play level between groups was not significant.
Reynell Receptive Language
The group to which the children belonged had no impact on the rate of their receptive language improvement scores. Children in both groups improved their receptive language skills by approximately 17 months over the 9 months of the study and follow up (Kasari, Gulsrud, Paparella, Hellemann, & Berry, 2015, p. 560).
Reynell Expressive Language
The group to which the children belonged had no impact on the rate of their expressive language improvement scores. Children in both groups improved their receptive language skills by an average of 10 months over the 9 month time frame (Kasari, Gulsrud, Paparella, Hellemann, & Berry., 2015, p. 560).
Parent Stress Index
Parents in the PSI group reported statistically significant lower stress in the child-related domain. At follow up, more parents reported lower levels of stress in this domain, but there was no difference based on the group to which they belonged. Parents in the PSI and JASPER group reported insignificantly different levels of stress for the parent-related domain.
Classroom observations
Children in the JASPER group spent statistically significant more time jointly engaging with their teacher than their peers in the PEI group by the end of treatment. The children in the JASPER group increased from 5.7 minutes to 8.9 minutes jointly engaging with their teacher. Children in the PEI group increased from 6.9 minutes to 7.4 minutes.
Things to Consider
The external validity of the study is limited as the children were recruited from an early intervention program that they all attended. We all work with children who tend to come from a variety of settings and attend a variety of programs.
It’s exciting that children in the JASPER group made gains in functional play skills and achieved higher levels of play by the end of intervention. However, the gains did not remain significantly different than those who did not receive the treatment. The authors mention exploring providing parents with sessions after intervention to ensure that the carryover at home continues.
Carryover from Parents to Classroom
I did find it impressive that the children’s joint attention carried over to engaging with their teachers even though the children were learning the skills at home. Also noteworthy is that the children from the JASPER group continued to have higher joint attention at the time of follow up.
I love structure and routine, and I need to learn more about the JASPER program to develop my opinion of it. You can also find more information about it here. It even seems that there is a training you can complete for free. I think it’s important to give kids the lead with play, but I do think we as adults can effectively scaffold their play by using specific techniques that may reach them most. For a lot of kids, you might not have to think too hard to figure them out. However, as kids on the Spectrum process in a unique way, we always have to be open to learning how to most effectively communicate with and reach them also.
What Do You Think?
Have you heard of the JASPER model before? What other strategies or programs have you used to promote play skills for children on the Autism Spectrum?
References
Kasari, C., Gulsrud, A., Paparella, T., Hellemann, G., & Berry, K. (2015). Randomized comparative efficacy study of parent-mediated interventions for toddlers with autism. Journal of Consulting and Clinical Psychology,83(3), 554-563. doi:10.1037/a0039080